

Mocht u de informatie op kanker-actueel waarderen dan wilt u misschien ons ondersteunen met een donatie. We zijn en blijven een ANBI organisatie, ook in 2019 dus uw donatie is in principe aftrekbaar voor de belastingen. Ook kunt u korting krijgen bij verschillende bedrijven op voedingssupplementen.
22 december 2018: Bron: ASCO 2018
Aanvullend op onderstaande publicaties is er weer een nieuwe studie: A randomized study of temozolomide or temozolomide and capecitabine in patients with advanced pancreatic neuroendocrine tumors: A trial of the ECOG-ACRIN Cancer Research Group (E2211). gepubliceerd die aantoont dat de combinatie van capecitabine (Xeloda) en Temodal (temozolomide) voor inoperabele of uitgezaaide alvleesklierkanker vanuit endocriene afkomst (Pnets) voor heel goede resultaten zorgt.
Uit een gerandomiseerde fase II studie bij 144 patiënten (72 vs 72) met uitgezaaide alvleesklierkanker vanuit endocriene afkomst (Pnets) blijkt dat de overall overleving nog niet is bereikt in de CAPTEM groep tegenover 38 maanden in de controlegroep die alleen capecitabine - Xeloda kregen. De progressievrije ziekte verbeterde ook statistisch significant: 22.7 vs 14.4 maanden.
Hier de resultaten uit het abstract dat ook onderaan dit artikel staat:
Results: 144 patients were enrolled at 66 US sites between 8/2013 to 3/2016 to T (n = 72) or TC (n = 72) (intention to treat population). Median age, 62 years; women, 44%. Median PFS was 22.7 months for TC vs. 14.4 months for T (HR = 0.58, p = 0.023) and crossed the pre-specified protocol efficacy boundary. Median OS was 38.0 months for T and has not been reached for TC (HR = 0.41, p = 0.012). Median follow-up was 29 months. RR data will be presented at the meeting. The treatment was well-tolerated with expected AEs and higher rates in the combination arm.
Al in 2014 schreven we dit (zie verderop in dit artikel): CAPTEM , een combinatie behandeling van Xeloda - capecitabine met temozolomide - temodal zorgt voor spectaculaire resultaten bij patiënten met alvleesklierkanker (NET tumoren), schildkliertumoren en hypofyse tumoren ontstaan vanuit neuro-endocriene afkomst.
Zie dus hieronder voor meer over de CAPTEM aanpak
12 januari 2017:
Als aanvulling op onderstaand artikel lees dit volledige studierapport: Outcomes of patients treated with capecitabine and temozolamide for advanced pancreatic neuroendocrine tumors (PNETs) and non-PNETs. met uitstekende referentielijst die ook onderaan dit artikel staat en die bevestigt dat CAPTEM - een combinatie van capecitabine (Xeloda) plus temozolomide (temodal) een uitstekende behandeling is die de levensduur sterk verlengt, ook bij zwaar voorbehandelde patiënten, met uitgezaaide neuro endocriene tumoren (NET- tumoren) zowel gerelateerd aan alvleesklier als longen als darmen of andere organen.
Hier scanbeelden van een patiënt voor en na een CAPTEM behandeling. Tekst gaat onder foto verder.
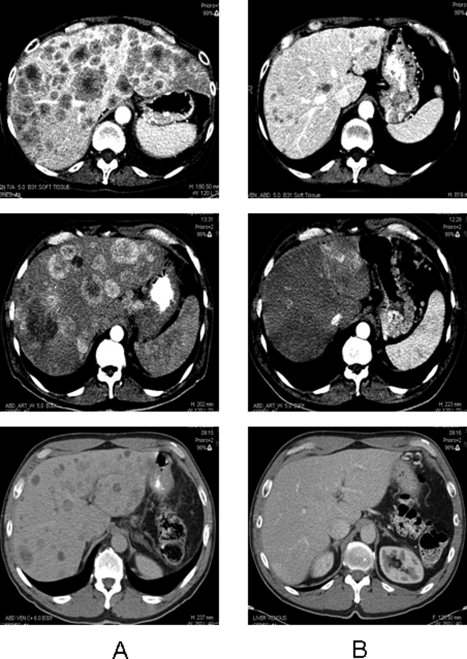
Foto boven: OS for the entire cohort (median 20.2 months, 95% CI, 9.02-33.37). OS, overall survival.
Een ander studierapport is het meest recente: The Role of Capecitabine/Temozolomide in Metastatic Neuroendocrine Tumors.
Conclusie
Veel vragen blijven hoe uitgezaaide NETs (neuro endocriene tumoren) te behandelen. Zoals wanneer te starten met een behandeling, frequentie van behandeling, is een gelijke behandeling voor alle vormen van NET's gewenst? De juiste keuze van gebruik van de Ki-67 mutatie en de voordelen van nieuwe recente behandelingen zoals bv. immuuntherapie.
De resultaten uit onze studie suggereren dat CAPTEM een effectieve behandeling kan zijn met verlenging van overall overleving voor patiënten met verschillende vormen en stadia van gevorderde uitgezaaide NET's - neuro endocriene tumoren. Hoewel er meer postspectieve studies nodig zijn is er wel bewijs dat CAPTEM een goede behandelingsoptie kan zijn voor patiënten met uitgezaaide PET's - neuro endocriene tumoren waar patiënten voor eerdere standaard behandelingen resistent bleken te zijn geworden.
Zie verder onderstaand artikel en klik eventueel door op studies in de referentielijsten onderaan dit artikel.
14 september 2015:
Als capecitabine plus temodal ingezet wordt als eerstelijns behandeling voor uitgezaaide alvleesklierNET zijn de resultaten extreem goed in vergelijking met standaard behandeling. 92% van de patiënten leefde nog na 2 jaar: zie volledige studierapport: First-line chemotherapy with capecitabine and temozolomide in patients with metastatic pancreatic endocrine carcinomas.
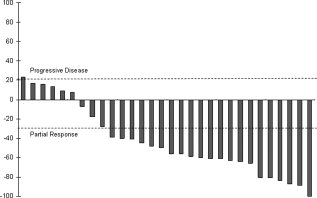
response van captem aanpak als eerstelijns aanpak
hier het volledige studierapprot van onderstaande studie: Outcomes of patients treated with capecitabine and temozolamide for advanced pancreatic neuroendocrine tumors (PNETs) and non-PNETs dat gratis is in te zien. de studie is uitgebreid naar een fase II studie waarbij ook patiënten worden opgenomen met vormen van kanker niet vanuit endocriene afkomst. Er worden nng steeds patiënten aangenomen: zie studieprotocol: https://clinicaltrials.gov/ct2/show/NCT01824875?term=NCT01824875&rank=1
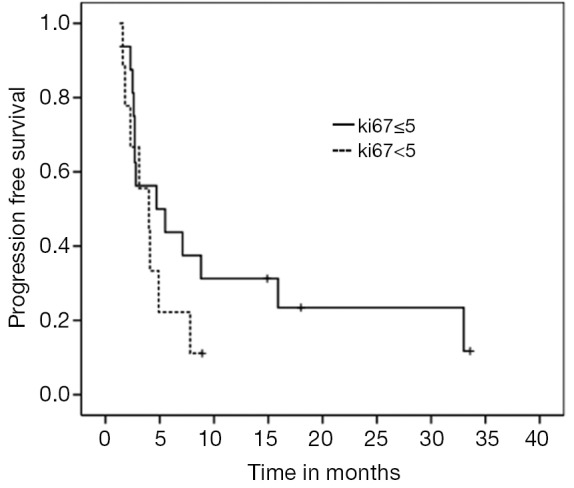
Bij de onderzoekers is er twijfel of capecitabine plus temodal ook werkt voor tumoren van niet neuro endocriene afkomst. Maar grafieken laten eigenlijk procentueel een zelfde effect zien op overall overleving.
Hier de twee grafieken, daaronder een uitgebreidere beschrijving van deze studie die zeer interessant is:
Overleving voor alle patienten
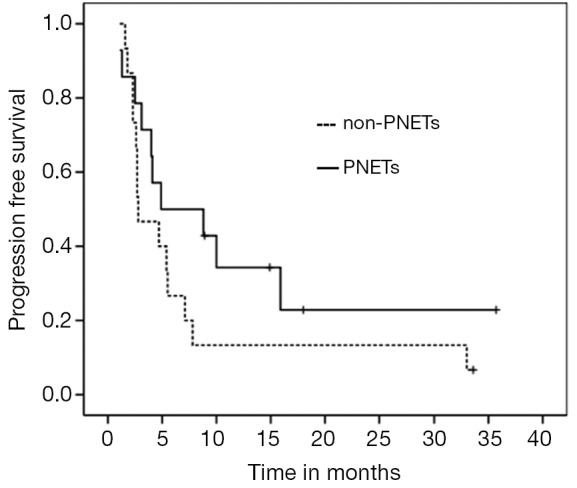
Overleving voor NET tumoren en niet NET tumoren
4 februari 2014: Bron: 2014 Gastrointestinal Cancers Symposium (GICS): Abstract 179. To be presented January 17, 2014
CAPTEM , een combinatie behandeling van Xeloda - capecitabine met temozolomide - temodal zorgt voor spectaculaire resultaten bij patiënten met alvleesklierkanker (NET tumoren), schildkliertumoren en hypofyse tumoren ontstaan vanuit neuro-endocriene afkomst.
Van de 28 deelnemende patiënten reageerde bijna iedereen (97%) positief op de behandeling met op z'n minst stabiele ziekte. 16 van de 28 deelnemers is nog steeds in leven waarvan de mediane progressievrije overlevingstijd inmiddels 29 maanden is maar deze kan nog langer worden omdat veel patiënten nog in leven zijn. Ook de bijwerkingen van deze aanpak blijken veel minder te zijn dan bij andere behandelingen van deze vorm van kanker.
Het bijzondere aan deze studie is ook dat alle patiënten vooraf de eerste lijnsbehandeling met octreotide(Sandostatine , Novartis) hebben gehad maar daaronder toch progressie van hun ziekte lieten zien. In feite waren deze patiënten dus uitbehandeld. En zoals verschillende oncologen lieten weten op de persconferentie, chemo bij deze vorm van kanker heeft weinig tot geen effect aangetoond tot nu toe. De reacties op het Gastrointestinal Cancers Symposium waren dan ook bijzonder positief omdat bij deze vorm van kanker er weinig andere opties tot behandelen zijn.
Dr. Fine van de Columbia University in New York staat aan de basis van deze studie. Hij onderzoekt al vanaf 2005 deze CAPTEM combinatie behandeling van capecitabine - xeloda plus temozolomide - temodal bij neuro endocriene tumoren.
Dr. Fine: "Temozolomide, bekend onder de merknaam Temodar, is een zogeheten cytotoxisch alkyleermiddel geïndiceerd voor gebruik bij patiënten met hersentumoren en uitgezaaide melanoom. Capecitabine - xeloda is een medicijn in tabeltvorm, wordt omgezet in het lichaam tot 5 - fluorouracil ( 5 - FU )en heeft bewezen de tumorgroei te vertragen en wordt gebruikt in een verscheidenheid van soorten kanker, zoals borstkanker en darmkanker.".
Volgens dr. Fine heeft deze combinatie zo'n grote kans van slagen omdat 5 - FU chemotherapie de "thymidine opslag" in de kankercel uitput (red: sorry maar weet niet goed wat dit precies is in het Nederlands) waardoor het celdodende aspect van temozolomide wordt versterkt.
Studieresultaten:
De studie is een zogeheten retrospectieve studie, uitgevoerd bij 28 patiënten. De studie begon al in 2005. De onderzoekers testten vooraf verschillende combinaties van medicijnen in het laboratorium voordat ze het protocol schreven dat wordt gebruikt in deze studie.
De patiënten kregen dagelijks capecitabine 1500 mg/m² gedurende 2 weken en dagelijkse temozolomide 150 tot 200 mg op dag 10 tot 14, met de volgende 2 weken geen medicijnen in een cyclus van 28 dagen. Alle deelnemende patiënten hadden goed of matig gedifferentieerde tumoren. Deze vertegenwoordigen de meeste gevallen van neuro-endocriene tumoren en staan bekend als resistent tegen een standaard eerstelijns en tweedelijns behandeling.
Overall 43 % van de deelnemende patienten reageerde positief op deze aanpak met capecitabine - xeloda en temolozomide - temodal (CAPTEM) en 54 % bereikten stabiele ziekte
CAPTEM bleek opvallend effectief bij de 3 patiënten met hypofyse tumoren, een moeilijk te behandelen neuro-endocriene tumor subtype en bekend staat als resistent te zijn tegen chemotherapie. Van de 3 patiënten met hypofyse tumoren - alle met toch progressie van de ziekte ondanks eerdere behandelingen met radiotherapie - bestraling, chemotherapie en chirurgie - bereikten 2 patiënten een volledige remissie met de behandeling (CAPTEM) en 1 patiënt bereikte een 75% reductie in tumorgrootte.
De twee complete remissies zijn heel bijzonder, aldus dr. Fine. Beide patienten waren in het eindstadium van hun ziekte en hadden al beademingsapparatuur nodig door de compressie van het ruggenmerg [veroorzaakt door de tumor]; Ze bereikten alle twee een volledige remissie, hadden de beademingsapparatuur niet meer nodig en zijn nu al bijna 4 jaar klinisch tumorvrij op een zogeheten onderhouds behandeling, aldus dr. Fine.
De combinatie behandeling bleek ook effectief bij de 11 patiënten met alvleesklierkanker vanuit neuro-endocriene oorsprong (NET tumoren). 55% bereikte stabiele ziekte, 36% een gedeeltelijke remissie (PR = 50% of meer vermindering van tumoromvang) .
De 2 patiënten met medullaire schildklier tumoren in deze studie bereikten beiden stabiele ziekte (100% respons).
Van de 12 patiënten met carcinoïde tumoren bereikten er 5 ( 41 % ) een vermindering van de tumoromvang van minstens 50% of meer. "Dit is heel ongebruikelijk ", aldus dr. Fine, omdat de respons op chemotherapie bij deze patiënten volgens de literatuur minder dan 3% is.
Voor de 28 studie patiënten was ten tijde van de analyse de mediane progressievrije overleving 22 maanden. De totale overlevingsgegevens zijn nog niet volledig te geven, maar mediane progressievrije overleving is meer dan 29 maanden op dit moment en 16 patiënten zijn nog steeds in leven en volgen nog steeds een zogeheten onderhoudsbehandeling.
Dr Fine zegt dat deze resultaten gunstig afsteken in vergelijking met octreotide, welke behandeling een respons geeft van ongeveer 6 % bij de verschillende typen van neuro-endocriene tumoren en ongeveer 30 % tot 40 % bereikt daarmee stabiele ziekte.
Tyrosine kinase remmers ( TKI's ), een klasse van geneesmiddelen voor neuro-endocriene tumoren waaronder sunitinib (Sutent , Pfizer), hebben volgens de literatuur een respons van minder dan 10 % en geven stabilisatie van de ziekte bij ongeveer 60 %. Met name klinische studies met TKI's zijn uitsluitend uitgevoerd bij patiënten met alvleesklierkanker vanuit neuro-endocriene oorsprong (NET tumoren).
Ongeveer 35% van de neuro-endocriene tumoren bestaat uit alvleeskliertumoren (NET tumoren) en deze zijn niet opgenomen in de lijst van patiënten met de meer behandelingsresistente carcinoide tumoren, welke ca. 55% deel uit maken van het totale aantal van neuro-endocriene tumoren, aldus dr. Fina op zijn persconferentie.
"De duur van de respons met CAPTEM is heel lang" aldus Dr Fine. "De langste overlevende patiënt in de CAPTEM studiegroep is nu al 8 jaar verder".
Bijwerkingen:
CAPTEM geeft in vergelijking met andere chemotherapieën voor deze groep van patiënten beduidend minder bijwerkingen. De meest voorkomende graad 3/4 bijwerkingen waren lymfopenie ( 35 % ) , hyperglycemie ( 6 % ) , thrombocytopenie ( 3 % ) , en diarree ( 3 % ) .
Conclusie:
"CAPTEM is de eerste behandeling met een bewezenwerkzaamheid in een breed scala van neuro-endocriene tumoren , waaronder carcinoïdtumoren, welke tot nu toe moeilijk te behandelen zijn." aldus dr. Fine.
Het behandelingsprotocol en fase II studie:
CAPTEM, de combinatie van capecitabine - xeloda en temozolomide - temodal wordt op dit moment onderzocht in een gerandomiseerde placebo gecontroleerde fase 2 studie. Klik hier voor het studieprotocol met e-mailadres en telefoonnummer van contactpersoon.
Er worden nog steeds patiënten aangenomen. Of zij ook patienten aannemen vanuit Europa durf ik niet te zeggen. Probleem is ook wel dat het een gerandomiseerde placebo gecontroleerde studie is (placebo is wel of niet xeloda, dus u kirjgt wel altijd temozolomide - temodal), waardoor als u wordt aangenomen u ook in de placebogroep kan terechtkomen.
Misschien beter uw behandelend arts vragen of u deze aanpak wellicht buiten studieverband kunt krijgen? Capecitabine en temozolomide zijn bekende reeds lang geregistreerde medicijnen, dus misschien wilt uw arts dit wel voorschrijven? Anders zou ik mytomorrows benaderen, misschien willen zij dit dan wel.
Dr Fine en Dr Krishnamurthi hebben verklaard geen relevante financiële belangen te hebben.
Het volledige studierapport: Capecitabine and temozolomide (CAPTEM) for metastatic, well-differentiated neuroendocrine cancers: The Pancreas Center at Columbia University experience opgemaakt maart 2013 is tegen in te zien. Het abstract van deze studie staat hieronder.
Van een andere studie met zelfde aanpak met alvleesklierkanker (NET tumoren) vanuit neuro-endocriene oorsprong en onderdeel van de hierboven beschreven studie is het volledige studierapport: A retrospective study of capecitabine/temozolomide (CAPTEM) regimen in the treatment of metastatic pancreatic neuroendocrine tumors (pNETs) after failing previous therapy wel gratis in te zien.
Het abstract daarvan staat ook hieronder. Referentielijst behorend bij CAPTEM studie staat onderaan dit artikel.
CAPTEM is highly active, well tolerated and may prolong survival in patients with well-differentiated, metastatic NET who have progressed on previous therapies
Capecitabine and temozolomide (CAPTEM) for metastatic, well-differentiated neuroendocrine cancers: The Pancreas Center at Columbia University experience.
Abstract
PURPOSE:
We evaluated the efficacy and safety of capecitabine and temozolomide (CAPTEM) in patients with metastatic neuroendocrine tumors (NETs) to the liver. This regimen was based on our studies with carcinoid cell lines that showed synergistic cytotoxicity with sequence-specific dosing of 5-fluorouracil preceding temozolomide (TMZ).
METHODS:
A retrospective review was conducted of 18 patients with NETs metastatic to the liver who had failed 60 mg/month of Sandostatin LAR™ (100%), chemotherapy (61%), and hepatic chemoembolization (50%). Patients received capecitabine at 600 mg/m(2) orally twice daily on days 1-14 (maximum 1,000 mg orally twice daily) and TMZ 150-200 mg/m(2) divided into two doses daily on days 10-14 of a 28-day cycle. Imaging was performed every 2 cycles, and serum tumor markers were measured every cycle.
RESULTS:
Using RECIST parameters, 1 patient (5.5%) with midgut carcinoid achieved a surgically proven complete pathological response (CR), 10 patients (55.5%) achieved a partial response (PR), and 4 patients (22.2%) had stable disease (SD). Total response rate was 61%, and clinical benefit (responders and SD) was 83.2%. Of four carcinoid cases treated with CAPTEM, there was 1 CR, 1 PR, 1 SD, and 1 progressive disease. Median progression-free survival was 14.0 months (11.3-18.0 months). Median overall survival from diagnosis of liver metastases was 83 months (28-140 months). The only grade 3 toxicity was thrombocytopenia (11%). There were no grade 4 toxicities, hospitalizations, opportunistic infections, febrile neutropenias, or deaths.
CONCLUSIONS:
CAPTEM is highly active, well tolerated and may prolong survival in patients with well-differentiated, metastatic NET who have progressed on previous therapies.
- PMID:
- 23370660
- [PubMed - indexed for MEDLINE]
A Retrospective Study of Capecitabine/Temozolomide (CAPTEM) Regimen in the Treatment of Metastatic Pancreatic Neuroendocrine Tumors (pNETs) after Failing Previous Therapy
JOP. J Pancreas (Online) 2013 Sep 10; 14(5):498-501.
Muhammad Wasif Saif1, Kristin Kaley2, Marianne Brennan2, Marie Carmel Garcon3, Gladys Rodriguez3, Teresa Rodriguez3
1Section of GI Cancers and Experimental Therapeutics, Tufts University School of Medicine. Boston, MA, USA. 2Yale School of Medicine. New Haven, CT, USA. 3Columbia University Medical Center. New York, NY, USA
ABSTRACT
Context Pancreatic neuroendocrine tumors (pNETs) are notoriously resistant to currently available chemotherapy agents. Preclinical data has suggested synergy between temozolomide and capecitabine.
Objective To report a retrospective data on the efficacy and safety of capecitabine and temozolomide (CAPTEM regimen) in patients with metastatic pancreatic neuroendocrine tumors (pNETs) who have failed prior therapies.
Methods We reviewed the medical records of 7 patients with metastatic pNETs who had had progressive cancer prior to treatment despite therapy, including long-acting release octreotide (60 mg/month), chemotherapy and hepatic chemoembolization. Capecitabine was administered at a flat dose of 1,000 mg orally twice daily on days 1-14 and temozolomide 200 mg/m2 was given in two divided doses daily on days 10-14 of a 28-day cycle. Tumor assessments were repeated every two cycles and serum tumor markers were measured every cycle. Response to treatment was assessed using Response Evaluation Criteria in Solid Tumors (RECIST) parameters, and toxicity was graded using the National Cancer Institute Common Terminology Criteria for Adverse Events (CTCAE), version 3.0.
Results Among 7 patients treated, three patients achieved a partial response, and two patients had stable disease. Total response rate was 43%, and clinical benefit (responders and stable disease) was 71%. Median duration of response was 8 months (range: 4-12 months). Grade 3 and 4 toxicities included grade 3 thrombocytopenia in one patient and grade 3 fatigue in one patient. The most common toxicities were grade 1 and 2 neutropenia, grade 1 fatigue, grade 1 and 2 hand-foot syndrome.
Conclusions Our retrospective study showed that modified CAPTEM regimen was well-tolerated and produced comparable response to historical data in neuroendocrine tumors, including pNETs. Our study is unique as it only included patients with pNETs. Further prospective studies are warranted to evaluate the combination of CAPTEM regimen with targeted therapies in pNETs.
References CAPTEM study
References
1. Dimou AT, Syrigos KN and Saif MW. Neuroendocrine tumors of the pancreas: what's new. Highlights from the "2010 ASCO Gastrointestinal Cancers Symposium". Orlando, FL, USA. January 22-24, 2010. JOP. J Pancreas (Online) 2010; 11:135-8. [PMID 20208321]
2. Yao JC, Hassan M, Phan A, Dagohoy C, Leary C, Mares JE, et al. One hundred years after "carcinoid": epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in the United States. J Clin Oncol 2008; 26:3063-72. [PMID 18565894]
3. Stevenson R, Libutti SK, Saif MW. Novel agents in gastroenteropancreatic neuroendocrine tumors. JOP. J Pancreas (Online) 2013; 14:152-4. [PMID 23474560]
4. Oberstein PE, Remotti H, Saif MW, Libutti SK. Pancreatic neuroendocrine tumors: entering a new era. JOP. J Pancreas (Online) 2012; 13:169-73. [PMID 22406593]
5. Cheng PN, Saltz LB. Failure to confirm major objective antitumor activity for streptozocin and doxorubicin in the treatment of patients with advanced islet cell carcinoma. Cancer 1999; 86:944-8. [PMID 10491519]
6. Kulke MH, Stuart K, Enzinger PC, Ryan DP, Clark JW, Muzikansky A, et al. Phase II study of temozolomide and thalidomide in patients with metastatic neuroendocrine tumors. J Clin Oncol 2006; 24: 401-6. [PMID 16421420]
7. Kulke MH, Stuart K, Earle CC, Bhargava P, Clark JW, Enzinger PC, et al. A phase II study of temozolomide and bevacizumab in patients with advanced neuroendocrine tumors. J Clin Oncol 2006; 24(18S): Abstract 4044.
8. Murakami J, Lee YJ, Kokeguchi S, Tsujigiwa H, Asaumi J, Nagatsuka H, et al. Depletion of O6-methylguanine -DNA methyltransferase by O6-benzylguanine enhances 5 -FU cytotoxicity in colon and oral cancer cell lines. Oncol Rep 2007; 17:1461-7. [PMID 17487405]
9. Isacoff WH, Moss RA, Pecora AL, Fine RL. Temozolomide/capecitabine therapy for metastatic neuroendocrine tumors of the pancreas. A retrospective review. J Clin Oncol 2006; 24(18S): Abstract 14023.
10. Strosberg JR, Fine RL, Choi J, Nasir A, Coppola D, Chen DT, et al. First-line chemotherapy with capecitabine and temozolomide in patients with metastatic pancreatic endocrine carcinomas. Cancer 2011; 117:268-75. [PMID 20824724]
11. Julka PK, Doval DC, Gupta S, Rath GK. Response assessment in solid tumours: a comparison of WHO, SWOG and RECIST guidelines. Br J Radiol 2008; 81:444-9. [PMID 18316345]
12. Cancer Therapy Evaluation Program. Common Terminology Criteria for Adverse Events (CTCAE) v4.0. National Cancer Institute at the National Institute of Health: Bethesda, MD, USA.
13. Rinke A, Müller HH, Schade-Brittinger C, Klose KJ, Barth P, Wied M, et al. Placebo-controlled, double-blind, prospective, randomized study on the effect of octreotide LAR in the control of tumor growth in patients with metastatic neuroendocrine midgut tumors: a report from the PROMID Study Group. J Clin Oncol 2009; 27:4656-63. [PMID 19704057]
14. Oberstein PE and Saif MW. Safety and efficacy of everolimus in adult patients with neuroendocrine tumors. Clin Med Insights Oncol 2012; 6:41-51. [PMID 22253554]
15. Yao JC, Shah MH, Ito T, Bohas CL, Wolin EM, Van Cutsem E, et al. Everolimus for advanced pancreatic neuroendocrine tumors. N Engl J Med 2011; 364:514-23. [PMID 21306238]
16. Raymond E, Dahan L, Raoul JL, Bang YJ, Borbath I, Lombard-Bohas C, et al. Sunitinib malate for the treatment of pancreatic neuroendocrine tumors. N Engl J Med 2011; 364:501-13. [PMID 21306237]
CAPTEM could potentially be an option for patients with advanced NETs who have progressed on standard treatment.
The Role of Capecitabine/Temozolomide in Metastatic Neuroendocrine Tumors
- Robert A. Ramireza,
- David T. Beyerb,
- Aman Chauhanc,
- J. Philip Boudreauxb,
- Yi-Zarn Wangb and
- Eugene A. Wolteringb
+ Author Affiliations
- Correspondence: Robert A. Ramirez, D.O., Neuroendocrine Tumor Program, Ochsner Medical Center, 200 West Esplanade Avenue, Suite 200, Kenner, Louisiana 70065, USA. Telephone: 504-464-8500; E-Mail: robert.ramirez@ochsner.org
- Received November 19, 2015.
- Accepted February 22, 2016.
- Published online before print May 25, 2016.
-
Disclosures of potential conflicts of interest may be found at the end of this article.
Abstract
Background.
Neuroendocrine tumors (NETs) are commonly treated with multimodality therapy. The combination of capecitabine and temozolomide (CAPTEM) has been suggested as a treatment option for patients with metastatic NETs. We present our experience with CAPTEM.
Methods.
Data on NET patients who were placed on CAPTEM and received at least one cycle were obtained from a Velos eResearch database. Response rate was calculated by RECIST 1.1. Overall survival and progression-free survival (PFS) were calculated by the Kaplan-Meier survival method.
Results.
A total of 29 patients (17 male and 12 female) were included. Median age at CAPTEM initiation was 58 years (range: 26–77). Primary tumors included 9 small bowel (31%), 15 pancreas (52%), 3 lung (10%), and 2 rectum (7%). Median number of CAPTEM cycles was 8 (range: 1–55). Partial response occurred in 5 patients (5 of 29, 17%); 14 patients (14 of 29, 48%) had stable disease, and 10 patients (10 of 29, 34%) had progressive disease. A total of 3 (20%) and 5 (33%) pancreatic NETs experienced partial response and stable disease, respectively. A total of 2 (14%) and 9 (64%) nonpancreatic NETs experienced partial response and stable disease, respectively. Partial response was noted in 1 patient (13%) and stable disease in 5 patients (63%) with Ki-67 values of less than 2%. In patients with Ki-67 values of 2%–20%, partial response was noted in 3 (19%) and stable disease in 8 (50%). Partial response and stable disease were noted in 1 patient each (20%) with Ki-67 values greater than 20%. Median PFS was 12 months. Adverse reactions caused dose reductions in 24% of patients.
Conclusion.
Although adverse reactions were experienced, most patients tolerated this regimen. CAPTEM should be considered as a reasonable treatment option for metastatic NET patients.
Implications for Practice:
The role of chemotherapy in neuroendocrine tumors has evolved in recent years. The results of this study suggest that the combination of capecitabine and temozolomide provides an adequate treatment option and may prolong survival in patients with a wide variety of metastatic neuroendocrine tumors. Although prospective data are needed, this research adds to the abundance of retrospective experience with this combination that appears to show that capecitabine and temozolomide could potentially be an option for patients with advanced neuroendocrine tumors who have progressed on standard treatment.
References
The ECOG-ACRIN study E2211 of 144 patients with advanced pancreatic neuroendocrine tumors (Pnets), presented by Kunz et al demonstrated that patients randomized to the doublet rather than single-agent temozolomide had a significant improvement in progression-free survival (22.7 vs 14.4 months) and overall survival (not reached vs 38.0 months)
A randomized study of temozolomide or temozolomide and capecitabine in patients with advanced pancreatic neuroendocrine tumors: A trial of the ECOG-ACRIN Cancer Research Group (E2211).
Background: Patients with advanced pancreatic neuroendocrine tumors (pNETs) have few treatment options that yield objective tumor regression. Somatostatin analogues, everolimus, and sunitinib yield prolonged progression-free survival (PFS) but low response rates (RRs). Retrospective and small, prospective studies suggest that temozolomide-based therapies may have activity and the combination of temozolomide and capecitabine (TC) is associated with high RRs and relative long PFS. However, there are no randomized, prospective studies of these agents and this trial was initiated to establish a role for the combination of TC.
Methods: E2211 was a two-arm, randomized, phase II trial comparing T (200 mg/m2 PO QD days 1-5) vs. TC (T 200 mg/m2 PO QD days 10-14; C 750 mg/m2 PO BID days 1-14) in patients with advanced pNETs. Eligibility criteria included: metastatic or unresectable, low or intermediate grade pNETs, progression within preceding 12 months, and no prior T, C, DTIC, or 5-FU. The primary endpoint was PFS; secondary endpoints were Overall Survival (OS), RR, safety, and predictive value of MGMT as evaluated by immunohistochemistry and promoter methylation. This trial had at least 81% power to detect a difference in median PFS of 9 vs. 14 months (hazard ratio of 0.64) using a two-sided log-rank test at the 0.20 significance level.
Results: 144 patients were enrolled at 66 US sites between 8/2013 to 3/2016 to T (n = 72) or TC (n = 72) (intention to treat population). Median age, 62 years; women, 44%. Median PFS was 22.7 months for TC vs. 14.4 months for T (HR = 0.58, p = 0.023) and crossed the pre-specified protocol efficacy boundary. Median OS was 38.0 months for T and has not been reached for TC (HR = 0.41, p = 0.012). Median follow-up was 29 months. RR data will be presented at the meeting. The treatment was well-tolerated with expected AEs and higher rates in the combination arm. Conclusions: In E2211, TC was associated with improved PFS and OS compared to T alone in advanced low or intermediate grade pNETs. This is the first prospective randomized trial of these agents and shows the longest PFS reported for pNET-directed therapy. Clinical trial information: NCT01824875
Plaats een reactie ...
1 Reactie op "CAPTEM een combinatie van Xeloda - capecitabine met temozolomide - temodal zorgt voor spectaculaire resultaten (97% minimaal stabiele ziekte) bij patiënten met alvleesklierkanker (NET3), carcinoid, schildkliertumoren en hypofyse tumoren"
Gerelateerde artikelen
- Immuuntherapie met pembrolizumab geeft weinig tot geen effect bij uitgezaaide neuro endocriene tumoren en andere aanpak lijkt noodzakelijk voor deze vorm van kanker
- CAPTEM een combinatie van Xeloda - capecitabine met temozolomide - temodal zorgt voor spectaculaire resultaten (97% minimaal stabiele ziekte) bij patiënten met alvleesklierkanker (NET3), carcinoid, schildkliertumoren en hypofyse tumoren
- Carcinoid Syndroom - Carcinoide tumoren informatie algemeen
- Everolimus plus octreotide (LAR) verbetert voor gevorderde neuro endocriene tumoren - carcinoidsyndroom - met een laag en gemiddeld stadium de progressievrije overlevingstijd
- Peptide Receptor Radionuclide Therapie (PRRT) geeft uitstekende resultaten - 4 tot 6 jaar langere overleving - bij patiënten met neuro endocriene tumoren
- Sandostatine LAR (langwerkend octreotide-acetaat). werkt uitstekend bij patiënten met Carcinoid Syndroom - Carcinoide tumoren, aldus studie uit Engeland, maar wordt ook in Rotterdam - Erasmus Medisch Centrum toegepast.
- Hoge dosis radioactief jodium - ook wel bekend als inwendige bestraling - als aanvulling gegeven aan patiënten met uitgezaaide carcinoid, waarbij alle andere medicijnen en aanpak niets hielp geeft significant betere resultaten op langere overlevingstijd
Mvg Astrid Beekman