

Helpt u ons aan 500 donateurs om kanker-actueel online te kunnen houden?
31 juli 2023: zie ook dit artikel: https://kanker-actueel.nl/niraparib-zejula-als-onderhoudsbehandeling-bij-gevorderde-eierstokkanker-geeft-een-veel-langere-progressievrije-overleving-bij-zowel-patienten-met-brca-gemuteerde-eierstokkanker-als-bij-niet-brca-gemuteerd.html
1 augustus 2018: lees ook dit artikel:
4 april 2018: zie ook dit artikel:
6 november 2016: Lees ook dit artikel:
Lees ook dit artikel:
30 september 2017: Lees ook dit artikel:
20 maart 2017: Bron: Het 2017 Society for Gynecologic Oncology (SGO) Annual Meeting on Women's Cancer,
Ook de eindresultaten van de ENGOT-OV16/NOVA studie, niraparib bij gevorderde eierstokkanker bevestigt de goede resultaten uit de eerste analyse, zie hieronder artikel van 6 november 2016.
Resultaten tonen aan dat een behandeling met niraparib ziekte progressie en de sterfte met 73% vermindert bij eierstokkankerpatiënten met de BRCA mutaties BRCA 1 en 2 (HR = 0.27) en met 55% bij eierstokkankerpatiënten zonder BRCA 1 en 2 mutaties. (HR = 0.45).
Op de SGO afgelopen week werden deze resultaten gepubliceerd. Tekst gaat verder onder poster
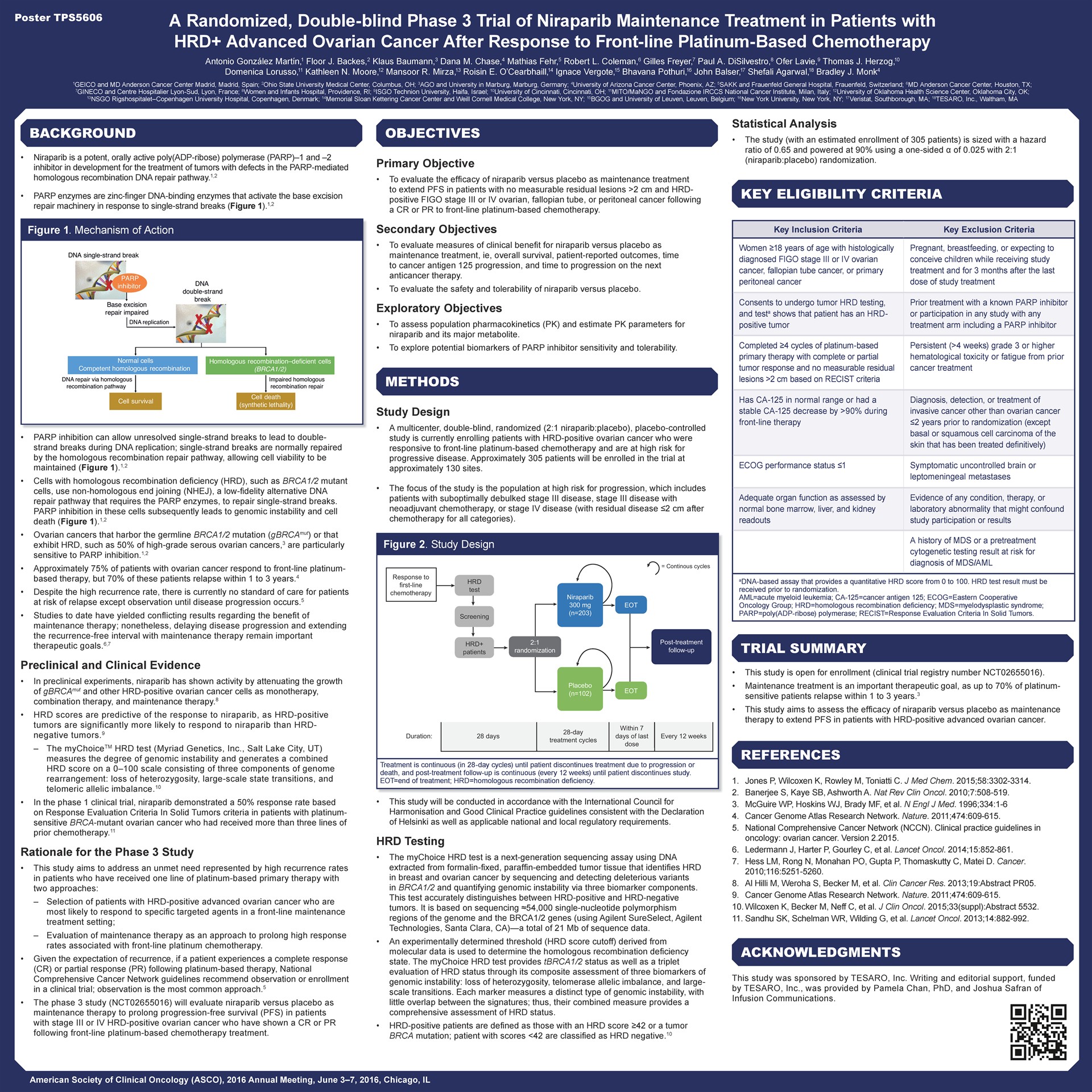
Phase III ENGOT-OV16/NOVA Trial Results
Ga naar deze website: http://www.ascopost.com/News/52430 en bekijk de video van de presentatie:
6 november 2016: Lees ook dit artikel:
12 oktober 2016: Bron; ESMO 2016 en NEJM October 8, 2016DOI: 10.1056/NEJMoa1611310
De PARP remmer niraparib verlengt de tweede progressievrije periode met 15,5 maand (21 maanden versus 5,5 maanden) in vergelijking met een placebo. Nirapanib werd toegevoegd aan de chemo na een recidief van eierstokkanker die gevoelig bleek voor op platinum gebaseerde chemo en welke een BRCA 1 of 2 mutatie bij zich droegen. Maar ook bij geen BRCA mutaties maar wel andere DNA mutaties werkte niraparib ook nog beduidend beter dan een placebo: progressievrije tijd steeg met ca. 8 maanden (12.9 vs 3.8).
Dit blijkt uit de resultaten uit de ENGOT-OV16/NOVA studie gepresenteerd door hoofdonderzoeker Mansoor Raza Mirza, MD op ESMO 2016 European Society for Medical Oncology in Copenhagen (Abstract LBA3_PR), en tegeljkertijd gepubliceerd in The New England Journal of Medicine.
Vergeleken met andere PARP remmers zoals olaparib zijn deze resultaten nog beter dan bij olaparib, aldus de onderzoekers. En heel veel beter in vergelijking met avastin - bevacizumab.
“The current options for maintenance therapy in the European Union (EU) are bevacizumab —which can only be given once and improves progression-free survival by just a few months—and the PARP inhibitor olaparib , which is only approved in patients with a germline BRCA mutation (about 10%–15% of ovarian cancer patients). No maintenance therapy is approved outside the EU,” said lead author Mansoor Raza Mirza, MD, Chief Oncologist at Rigshospitalet, Copenhagen University Hospital and Medical Director of the Nordic Society of Gynaecological Oncology.
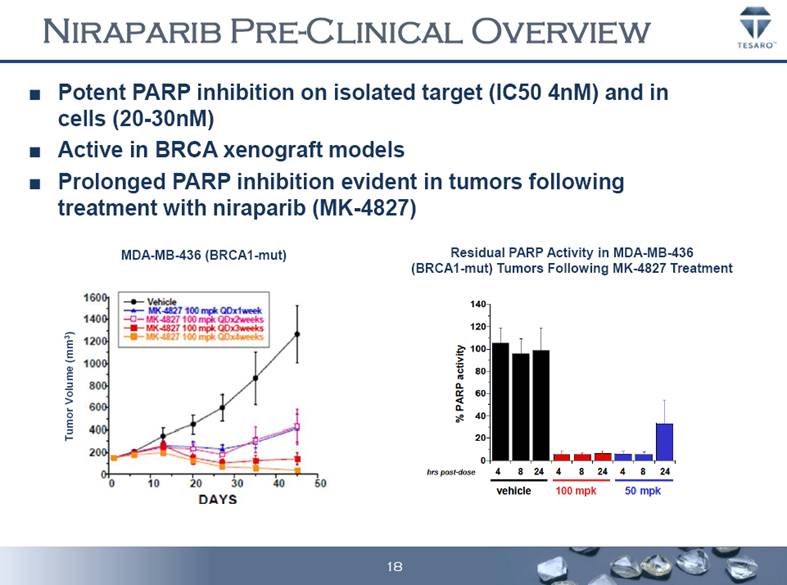
De grafieken met de resultaten uit het studierapport zijn te klein om hier weer te geven maar hier een grafiek uit eerdere klinische studies met niraparib:
Kernpunten uit de studie waren en ik vertaal ze maar niet want het eenvoudige Engels is voor de meesten wel te begrijpen neem ik aan:
Het volledige studierapport: Niraparib Maintenance Therapy in Platinum-Sensitive, Recurrent Ovarian Cancer ia gratis n te zien.
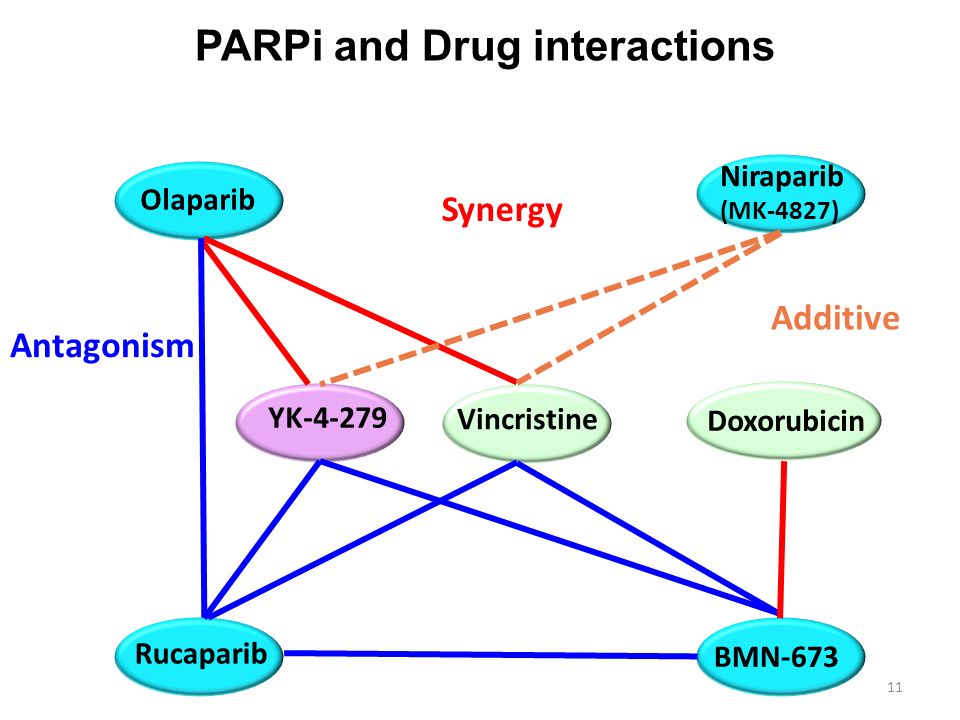
Foto boven: Werkingsmechanisme van PARP remmers
Hier het abstract van de studie:
Niraparib significantly improves outcomes in platinum-sensitive recurrent ovarian cancer
Niraparib Maintenance Therapy in Platinum-Sensitive, Recurrent Ovarian Cancer
October 8, 2016DOI: 10.1056/NEJMoa1611310
Background
Niraparib is an oral poly(adenosine diphosphate –ribose) polymerase (PARP) 1/2 inhibitor that has shown clinical activity in patients with ovarian cancer. We sought to evaluate the efficacy of niraparib versus placebo as maintenance treatment for patients with platinum-sensitive, recurrent ovarian cancer.
Methods
In this randomized, double-blind, phase 3 trial, patients were categorized according to the presence or absence of a germline BRCA mutation (gBRCA cohort and non-gBRCA cohort) and the type of non-gBRCA mutation and were randomly assigned in a 2:1 ratio to receive niraparib (300 mg) or placebo once daily. The primary end point was progression-free survival.
Results
Of 553 enrolled patients, 203 were in the gBRCA cohort (with 138 assigned to niraparib and 65 to placebo), and 350 patients were in the non-gBRCA cohort (with 234 assigned to niraparib and 116 to placebo). Patients in the niraparib group had a significantly longer median duration of progression-free survival than did those in the placebo group, including 21.0 vs. 5.5 months in the gBRCA cohort (hazard ratio, 0.27; 95% confidence interval , 0.17 to 0.41), as compared with 12.9 months vs. 3.8 months in the non-gBRCA cohort for patients who had tumors with homologous recombination deficiency (HRD) (hazard ratio, 0.38; 95% CI, 0.24 to 0.59) and 9.3 months vs. 3.9 months in the overall non-gBRCA cohort (hazard ratio, 0.45; 95% CI, 0.34 to 0.61; P<0.001 for all three comparisons). The most common grade 3 or 4 adverse events that were reported in the niraparib group were thrombocytopenia (in 33.8%), anemia (in 25.3%), and neutropenia (in 19.6%), which were managed with dose modifications.
Conclusions
Among patients with platinum-sensitive, recurrent ovarian cancer, the median duration of progression-free survival was significantly longer among those receiving niraparib than among those receiving placebo, regardless of the presence or absence of gBRCA mutations or HRD status, with moderate bone marrow toxicity. (Funded by Tesaro; ClinicalTrials.gov number, NCT01847274.)
-
References
-
1
SEER Cancer Statistics Review (CSR) 1975–2013. Bethesda, MD: National Cancer Institute, 2016 (http://seer.cancer.gov/csr/1975_2013/).
-
2
GLOBOCAN 2012 v1.0, estimated cancer incidence, mortality and prevalence worldwide: IARC CancerBase no. 11. Lyon, France: International Agency for Research on Cancer, 2013 (http://publications.iarc.fr/Databases/Iarc-Cancerbases/Globocan-2012-Estimated-Cancer-Incidence-Mortality-And-Prevalence-Worldwide-In-2012-V1-0-2012).
-
3
Hanker LC, Loibl S, Burchardi N, et al. The impact of second to sixth line therapy on survival of relapsed ovarian cancer after primary taxane/platinum-based therapy. Ann Oncol 2012;23:2605-2612
CrossRef | Web of Science | Medline
-
4
Jones P, Altamura S, Boueres J, et al. Discovery of 2-4-[(3S)-piperidin-3-yl]phenyl-2H-indazole-7-carboxamide (MK-4827): a novel oral poly(ADP-ribose)polymerase (PARP) inhibitor efficacious in BRCA-1 and -2 mutant tumors. J Med Chem 2009;52:7170-7185
CrossRef | Web of Science | Medline
-
5
Audeh MW, Carmichael J, Penson RT, et al. Oral poly(ADP-ribose) polymerase inhibitor olaparib in patients with BRCA1 or BRCA2 mutations and recurrent ovarian cancer: a proof-of-concept trial. Lancet 2010;376:245-251
CrossRef | Web of Science | Medline
-
6
Fong PC, Boss DS, Yap TA, et al. Inhibition of poly(ADP-ribose) polymerase in tumors from BRCA mutation carriers. N Engl J Med 2009;361:123-134
Free Full Text | Web of Science | Medline
-
7
Kummar S, Ji J, Morgan R, et al. A phase I study of veliparib in combination with metronomic cyclophosphamide in adults with refractory solid tumors and lymphomas. Clin Cancer Res 2012;18:1726-1734
CrossRef | Web of Science | Medline
-
8
Ledermann J, Harter P, Gourley C, et al. Olaparib maintenance therapy in platinum-sensitive relapsed ovarian cancer. N Engl J Med 2012;366:1382-1392
Free Full Text | Web of Science | Medline
-
9
Gelmon KA, Tischkowitz M, Mackay H, et al. Olaparib in patients with recurrent high-grade serous or poorly differentiated ovarian carcinoma or triple-negative breast cancer: a phase 2, multicentre, open-label, non-randomised study. Lancet Oncol 2011;12:852-861
CrossRef | Web of Science | Medline
-
10
Sandhu SK, Schelman WR, Wilding G, et al. The poly(ADP-ribose) polymerase inhibitor niraparib (MK4827) in BRCA mutation carriers and patients with sporadic cancer: a phase 1 dose-escalation trial. Lancet Oncol 2013;14:882-892
CrossRef | Web of Science | Medline
-
11
du Bois A, Reuss A, Pujade-Lauraine E, et al. European Network of Gynaecological Oncological Trial Groups’ requirements for trials between academic groups and industry partners — first update 2015. Int J Gynecol Cancer 2015;25:1328-1330
CrossRef | Web of Science | Medline
-
13
Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer 2009;45:228-247
CrossRef | Web of Science | Medline
-
Gerelateerde artikelen
- Niraparib - Zejula als onderhoudsbehandeling bij gevorderde eierstokkanker geeft een veel langere progressievrije overleving bij zowel patiënten met BRCA-gemuteerde eierstokkanker als bij niet BRCA-gemuteerd
- niraparib plus bevacizumab (Avastin) zonder chemo of gegeven in chemovrije periode verdubbelt bij eierstokkanker ziektevrije tijd en ziektevrije overleving steeg met 26 procent (79 vs 53 procent)
- Niraparib geeft zeer goede resultaten bij recidief van gevorderde eierstokkanker die eerder gevoelig bleek voor op platinum gebaseerde chemo copy 1
- Parpremmers Olaparib en niraparib gegeven als onderhoudsbehandeling bij gevorderde chemo gevoelige eierstokkanker heeft geen negatief effect op kwaliteit van leven en geeft wel betere overall overleving
- PARP remmers zoals olaparib zouden in vroeger stadium van eierstokkanker en andere vormen van kanker met BRCA mutaties moeten worden ingezet want teveel chemokuren verminderen kans op aanslaan van de behandeling, stellen oncologen n.a.v. diverse studies
- Talazoparib, een PARP remmer, wordt in veel studies bij veel verschillende vormen van kanker en in combinatie met andere medicijnen onderzocht en geeft veelbelovende resultaten copy 1
- Olaparib plus Bevacizumab als eerstelijns onderhoudsbehandeling voor eierstokkanker geeft betere progressievrije ziekte dan placebo ongeacht BRCA status.
- Olaparib als onderhoudsbehandeling voor BRCA 1/2 uitgezaaide platinum gevoelige eierstokkanker geeft 70 procent minder kans op overlijden in vergelijking met placebo
- Olaparib, een PARP remmer, verlengt ziektevrije en overall overleving in vergelijking met placebo bij eierstokkanker met BRCA 1 en 2
- Olaparib plus cedinarib lijkt doorbraak bij controle van vergevorderde eierstokkanker en verdubbelt progressievrije overleving van 9,2 maanden naar 17,7 maanden
- Parpremmer niraparib naast chemo en daarna als onderhoudsbehandeling verdubbelt mediane overall overleving in vergelijking met placebo
- Parpremmer Veliparib naast chemo gevolgd door veliparib alleen als onderhoudsbehandeling geeft betere overall overleving voor patienten met eierstokkanker stadium III en IV.
- Patienten met gevorderde eierstokkanker met een PARP-7 mutatie / expressie blijken veel betere mediane overall overleving te hebben (45 vs 16 maanden) dan zonder PARP-7 mutatie / expressie. copy 1
- Parpremmer rucaparib verdubbelt ziektevrije overleving (5 vs 11 en 13 maanden) bij chemo gevoelige eierstokkanker. Ook bij patienten zonder BRCA mutatie is rucaparib effectief
- PARP remmers zoals olaparib zouden in vroeger stadium van eierstokkanker en andere vormen van kanker met BRCA mutaties moeten worden ingezet
- BRCA - erfelijkheid: Combinatie van sapacitabine en seliciclib geeft een hoopvol therapeutisch effect bij zwaar voorbehandelde kankerpatienten met solide tumoren met onderliggende afwijkende erfelijke BCRA gen mutaties. copy 1
- PARP remmers zoals olaparib, niraparib en rucaparib zijn effectief zowel met als zonder BRCA mutaties, een overzicht
Plaats een reactie ...
Reageer op "Niraparib geeft zeer goede resultaten bij recidief van gevorderde eierstokkanker die eerder gevoelig bleek voor op platinum gebaseerde chemo copy 1"