

Helpt u ons aan 500 donateurs om kanker-actueel online te kunnen houden?
1 november 2018: Zie ook dit artikel:
1 augustus 2018: lees ook dit artikel:
4 april 2018: lees ook dit artikel:
en zie ook de artikelen in gerelateerde artikelen
4 april 2018: Bron: HOPA 2018
Rucaparib (RUBRACA) een zogeheten parpremmer verlengt als onderhoudsbehandeling de progressievrije overleving met meer dan 100 procent in vergelijking met een placebo bij vrouwen met een recidief van platinum-gevoelige (chemo gevoelig) eierstokkanker. De ziektevrije en progressievrije overleving in vergelijking met een placebo was beduidend beter voor rucaparib, 13,6 maanden vs 5,4 voor placebo bij alle deelnemende patiënten ongeacht hun BRCA status. Dus ook bij vrouwen met eierstokkanker die geen BRCA mutatie hebben zorgt rucaparib (RUBRACA) voor uitstekende resultaten.
Bij vrouwen met wel een BRCA mutatie status waren de resultaten nog beter, 16,6 maanden voor rucaparib versus 5,4 maanden voor placebo. Blijkt uit de ARIEL3 fase III studie.
Hier een grafiek van hoe de ARIEL studies zijn verlopen afgelopen jaren (tekst gaat verder onder grafiek) :
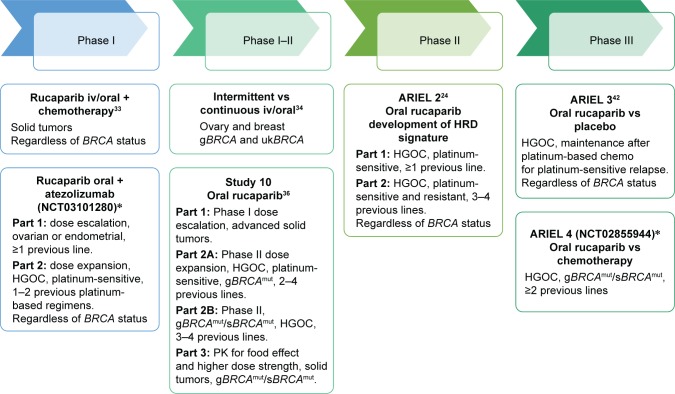
Bovenstaande en onderstaande grafiek komt uit een reviewstudie december 2017 over rucaparuib bij zowel eierstokkanker als borstkanker: Emerging treatment options for ovarian cancer: focus on rucaparib
Table 3
PFS/ORR by HRD sub-group with rucaparib in relapsed, platinum-sensitive high-grade ovarian carcinoma (ARIEL2 part 1)5
| HRD subgroups of high-grade ovarian cancer | Number of patients in each group | Median PFS, months (95% CI) | Hazard ratio | ORR | |
|---|---|---|---|---|---|
| RECIST, % (n, 95% CI) | RECIST/CA125, % (n, 95% CI) | ||||
| BRCA mutant | 40 | 12.8 (9.0–14.7) | 0.27, P<0.0001 | 80% (32, 64–91) | 85% (34, 70–94) |
| BRCA wild type and LOH high | 82 | 5.7 (5.3–7.6) | 0.62, P<0.011 | 29% (24, 20–40) | 44% (34, 33–55) |
| BRCA wild type and LOH low | 70 | 5.2 (3.6–5.5) | – | 10% (7, 4–20) | 20% (14, 11–31) |
Abbreviations: BRCA, breast and ovarian cancer susceptibility gene; CI, confidence interval; CA125, cancer antigen 125; HRD, homologous recombination repair deficiency; LOH, loss of heterozygosity; ORR, objective response rate; PFS, progression-free survival; RECIST, Response Evaluation Criteria In Solid Tumors (Version 1.1).
Uit de presentatie van de nieuwste studie op HOPA 2018:
Op basis van een intent-to-treat analyse was de mediane progressievrije overleving 10,8 maanden (95% betrouwbaarheidsinterval 8,3 - 11,4) met rucaparib, vergeleken met 5,4 maanden (95% betrouwbaarheidsinterval 5,3 - 5,5) voor placebo (P <.0001 ).
Van de 354 homologe recombinatie-deficiënte patiënten was de mediane progressievrije overleving met rucaparib 13,6 maanden (95% betrouwbaarheidsinterval 10,9 - 16,2) en 5,4 maanden voor placebo (95% betrouwbaarheidsinterval 5,1 - 5,6) (p <.0001).
Bij de 196 patiënten, specifiek met BRCA-mutaties, was de mediane progressievrije overleving voor rucaparib 16,6 maanden (95% betrouwbaarheidsinterval 13,4 - 22,9) en 5,4 maanden voor placebo (95% betrouwbaarheidsinterval 3,4 - 6,7) (P <.0001).
De meest gemelde aan de behandeling gerelateerde bijwerkingen waren misselijkheid en braken, evenals asthenie en bloedarmoede. De auteurs melden dat deze consistent zijn met eerdere studies van rucaparib. De bijwerkingen werden behandeld met profylactische en / of ondersteunende zorg, onderbrekingen in de behandeling en / of dosisverlagingen.
Conclusie:
Rucaparib effectively increases progression-free survival with high-grade, recurrent, platinum-sensitive ovarian cancer regardless of HRR status. They suggest that it could be considered as a new standard of care for women with platinum-sensitive ovarian cancer following a partial or complete response to second-line or later platinum-based chemotherapy.
Het volledige studierapport van de HOPA gepresenteerde studie is in december 2017 gepubliceerd in The Lancet: Rucaparib maintenance treatment for recurrent ovarian carcinoma after response to platinum therapy (ARIEL3): a randomised, double-blind, placebo-controlled, phase 3 trial en tegen betaling in te zien.
Hier het abstract van de studie met referentielijst van reviewstudie:
Rucaparib effectively increases progression-free survival with high-grade, recurrent, platinum-sensitive ovarian cancer regardless of HRR status. They suggest that it could be considered as a new standard of care for women with platinum-sensitive ovarian cancer following a partial or complete response to second-line or later platinum-based chemotherapy.
Rucaparib maintenance treatment for recurrent ovarian carcinoma after response to platinum therapy (ARIEL3): a randomised, double-blind, placebo-controlled, phase 3 trial
 Correspondence information about the author Prof Robert L Coleman*,
Correspondence information about the author Prof Robert L Coleman*, ARIEL3 investigators†
ARIEL3 investigators†Summary
Background
Rucaparib, a poly(ADP-ribose) polymerase inhibitor, has anticancer activity in recurrent ovarian carcinoma harbouring a BRCA mutation or high percentage of genome-wide loss of heterozygosity. In this trial we assessed rucaparib versus placebo after response to second-line or later platinum-based chemotherapy in patients with high-grade, recurrent, platinum-sensitive ovarian carcinoma.
Methods
In this randomised, double-blind, placebo-controlled, phase 3 trial, we recruited patients from 87 hospitals and cancer centres across 11 countries. Eligible patients were aged 18 years or older, had a platinum-sensitive, high-grade serous or endometrioid ovarian, primary peritoneal, or fallopian tube carcinoma, had received at least two previous platinum-based chemotherapy regimens, had achieved complete or partial response to their last platinum-based regimen, had a cancer antigen 125 concentration of less than the upper limit of normal, had a performance status of 0–1, and had adequate organ function. Patients were ineligible if they had symptomatic or untreated central nervous system metastases, had received anticancer therapy 14 days or fewer before starting the study, or had received previous treatment with a poly(ADP-ribose) polymerase inhibitor. We randomly allocated patients 2:1 to receive oral rucaparib 600 mg twice daily or placebo in 28 day cycles using a computer-generated sequence (block size of six, stratified by homologous recombination repair gene mutation status, progression-free interval after the penultimate platinum-based regimen, and best response to the most recent platinum-based regimen). Patients, investigators, site staff, assessors, and the funder were masked to assignments. The primary outcome was investigator-assessed progression-free survival evaluated with use of an ordered step-down procedure for three nested cohorts: patients with BRCA mutations (carcinoma associated with deleterious germline or somatic BRCA mutations), patients with homologous recombination deficiencies (BRCA mutant or BRCA wild-type and high loss of heterozygosity), and the intention-to-treat population, assessed at screening and every 12 weeks thereafter. This trial is registered with ClinicalTrials.gov, number NCT01968213; enrolment is complete.
Findings
Between April 7, 2014, and July 19, 2016, we randomly allocated 564 patients: 375 (66%) to rucaparib and 189 (34%) to placebo. Median progression-free survival in patients with a BRCA-mutant carcinoma was 16·6 months (95% CI 13·4–22·9; 130 [35%] patients) in the rucaparib group versus 5·4 months (3·4–6·7; 66 [35%] patients) in the placebo group (hazard ratio 0·23 [95% CI 0·16–0·34]; p<0·0001). In patients with a homologous recombination deficient carcinoma (236 [63%] vs 118 [62%]), it was 13·6 months (10·9–16·2) versus 5·4 months (5·1–5·6; 0·32 [0·24–0·42]; p<0·0001). In the intention-to-treat population, it was 10·8 months (8·3–11·4) versus 5·4 months (5·3–5·5; 0·36 [0·30–0·45]; p<0·0001). Treatment-emergent adverse events of grade 3 or higher in the safety population (372 [99%] patients in the rucaparib group vs 189 [100%] in the placebo group) were reported in 209 (56%) patients in the rucaparib group versus 28 (15%) in the placebo group, the most common of which were anaemia or decreased haemoglobin concentration (70 [19%] vs one [1%]) and increased alanine or aspartate aminotransferase concentration (39 [10%] vs none).
Interpretation
Across all primary analysis groups, rucaparib significantly improved progression-free survival in patients with platinum-sensitive ovarian cancer who had achieved a response to platinum-based chemotherapy. ARIEL3 provides further evidence that use of a poly(ADP-ribose) polymerase inhibitor in the maintenance treatment setting versus placebo could be considered a new standard of care for women with platinum-sensitive ovarian cancer following a complete or partial response to second-line or later platinum-based chemotherapy.
Funding
Clovis Oncology
Disclosure
YD is an investigator on clinical trials of olaparib and rucaparib, has participated in advisory boards for Clovis Oncology and AstraZeneca, has received research grant support from Clovis Oncology, and was involved in the preclinical and clinical development of rucaparib. Newcastle University receives royalties for rucaparib. The authors report no other conflicts of interest in this work.
References
Articles from International Journal of Women's Health are provided here courtesy of Dove Press
Plaats een reactie ...
1 Reactie op "Parpremmer rucaparib verdubbelt ziektevrije overleving (5 vs 11 en 13 maanden) bij chemo gevoelige eierstokkanker. Ook bij patienten zonder BRCA mutatie is rucaparib effectief"
Gerelateerde artikelen
- Niraparib - Zejula als onderhoudsbehandeling bij gevorderde eierstokkanker geeft een veel langere progressievrije overleving bij zowel patiënten met BRCA-gemuteerde eierstokkanker als bij niet BRCA-gemuteerd
- niraparib plus bevacizumab (Avastin) zonder chemo of gegeven in chemovrije periode verdubbelt bij eierstokkanker ziektevrije tijd en ziektevrije overleving steeg met 26 procent (79 vs 53 procent)
- Niraparib geeft zeer goede resultaten bij recidief van gevorderde eierstokkanker die eerder gevoelig bleek voor op platinum gebaseerde chemo copy 1
- Parpremmers Olaparib en niraparib gegeven als onderhoudsbehandeling bij gevorderde chemo gevoelige eierstokkanker heeft geen negatief effect op kwaliteit van leven en geeft wel betere overall overleving
- PARP remmers zoals olaparib zouden in vroeger stadium van eierstokkanker en andere vormen van kanker met BRCA mutaties moeten worden ingezet want teveel chemokuren verminderen kans op aanslaan van de behandeling, stellen oncologen n.a.v. diverse studies
- Talazoparib, een PARP remmer, wordt in veel studies bij veel verschillende vormen van kanker en in combinatie met andere medicijnen onderzocht en geeft veelbelovende resultaten copy 1
- Olaparib plus Bevacizumab als eerstelijns onderhoudsbehandeling voor eierstokkanker geeft betere progressievrije ziekte dan placebo ongeacht BRCA status.
- Olaparib als onderhoudsbehandeling voor BRCA 1/2 uitgezaaide platinum gevoelige eierstokkanker geeft 70 procent minder kans op overlijden in vergelijking met placebo
- Olaparib, een PARP remmer, verlengt ziektevrije en overall overleving in vergelijking met placebo bij eierstokkanker met BRCA 1 en 2
- Olaparib plus cedinarib lijkt doorbraak bij controle van vergevorderde eierstokkanker en verdubbelt progressievrije overleving van 9,2 maanden naar 17,7 maanden
- Parpremmer niraparib naast chemo en daarna als onderhoudsbehandeling verdubbelt mediane overall overleving in vergelijking met placebo
- Parpremmer Veliparib naast chemo gevolgd door veliparib alleen als onderhoudsbehandeling geeft betere overall overleving voor patienten met eierstokkanker stadium III en IV.
- Patienten met gevorderde eierstokkanker met een PARP-7 mutatie / expressie blijken veel betere mediane overall overleving te hebben (45 vs 16 maanden) dan zonder PARP-7 mutatie / expressie. copy 1
- Parpremmer rucaparib verdubbelt ziektevrije overleving (5 vs 11 en 13 maanden) bij chemo gevoelige eierstokkanker. Ook bij patienten zonder BRCA mutatie is rucaparib effectief
- PARP remmers zoals olaparib zouden in vroeger stadium van eierstokkanker en andere vormen van kanker met BRCA mutaties moeten worden ingezet
- BRCA - erfelijkheid: Combinatie van sapacitabine en seliciclib geeft een hoopvol therapeutisch effect bij zwaar voorbehandelde kankerpatienten met solide tumoren met onderliggende afwijkende erfelijke BCRA gen mutaties. copy 1
- PARP remmers zoals olaparib, niraparib en rucaparib zijn effectief zowel met als zonder BRCA mutaties, een overzicht
Ook de niraparib (Zejula) laat goede resultaten zien en schijnt al goedgekeurd te zijn door de EMA.
De vraag is nu: kunnen vrouwen die al eerder behandeld zijn voor eierstok kanker, BRCA-gendraagster zijn, en nog steeds kankervrij, profylactisch behandeld worden met dit middel? Want dat die kanker terugkomt is vrijwel zeker. Maar met dit middel, kan het nog even uitgesteld worden...
Mijn gynaecologe doet er vaag over...
Wie kan hier antwoord op geven?