

Helpt u ons aan 500 donateurs?
30 augustus 2021: zie ook dit artikel: https://kanker-actueel.nl/vitamine-d-suppletie-reguleert-postoperatieve-bloedwaarden-van-pd-l1-bij-patienten-met-spijsverteringskanker-en-verbetert-sterk-de-overall-overleving-van-patienten-met-de-hoogste-pd-l1-waarden.html
25 mei 2019: Bron: The Harvard Gazette:
Als aanvulling op onderstaand artikel van 13 juni 2017 lees dit persbericht:
Vitamin D may slow progression of metastatic colorectal cancer
“The results of our trial suggest an improved outcome for patients who received vitamin D supplementation, and we look forward to launching a larger trial to confirm these exciting and provocative findings,” said Charles Fuchs, formerly of Dana-Farber and now director of Yale Cancer Center, the senior author of the study.
13 juni 2017: Bron: ASCO 2017
Een hoge dosis vitamine D3 suppletie naast chemo vertraagt de progressie van uitgezaaide darmkanker veel beter dan een lage dosis vitamine D3. Dit blijkt uit een gerandomiseerde fase II studie bij totaal 139 patiënten met uitgezaaide darmkanker die voor de eerste keer een chemokuur (mFOLFOX6 = folinic acid , fluorouracil, en oxaliplatin) plus Avastin - bevacizumab.) kregen. Die dus nog niet eerder waren behandeld.
- In de groep patiënten die een hoge dosis vitamine D3 kregen (n = 69) bleek de mediane progressievrije tijd 13,1 maanden vergeleken met 11,2 maanden voor de lage dosisgroep (n = 70). Dat vertaalt zich in een 31% verminderd risico op ziekteprogressie. (unadjusted hazard ratio, 0.69; P = .04), aldus de onderzoekers.
- Controle over de ziekte in de groep met hoge doses was 96% tegen 84% in de lage dosisgroep (P = .05).
- De hoge dosis verhoogde de toxiciteit - bijwerkingen niet. In tegendeel er was ook significant minder ernstige diarree (graad 3 en 4) in de groep die de hoge doses kreeg (12% versus 1%; P = 0,02).
- De resultaten waren nog indrukwekkender omdat er een significant verschil was in lichamelijke gesteldheid tussen de twee studiegroepen die voor de lage dosisgroep betere scoorde: 60% van de lage dosisgroep had de best mogelijke lichamelijke conditie tegenover slechts 42% van de groep met een hoge dosis. Met andere woorden, de hoge dosis groep deed het beter, hoewel de patiënten fysiek minder fit waren dan in de vergelijkende groep die de lage dosisgroep vormde. Bv. meer patiënten uit de hoge dosis vitamine D groep waren in staat om alsnog een operatie te ondergaan na hun chemotherapie (11 tegen 6). Het verschil was echter niet statistisch significant (P = 0,19)
- De mediane follow-up was 16,9 maanden in de hoge dosisgroep en 17,9 maanden in de lage dosisgroep.
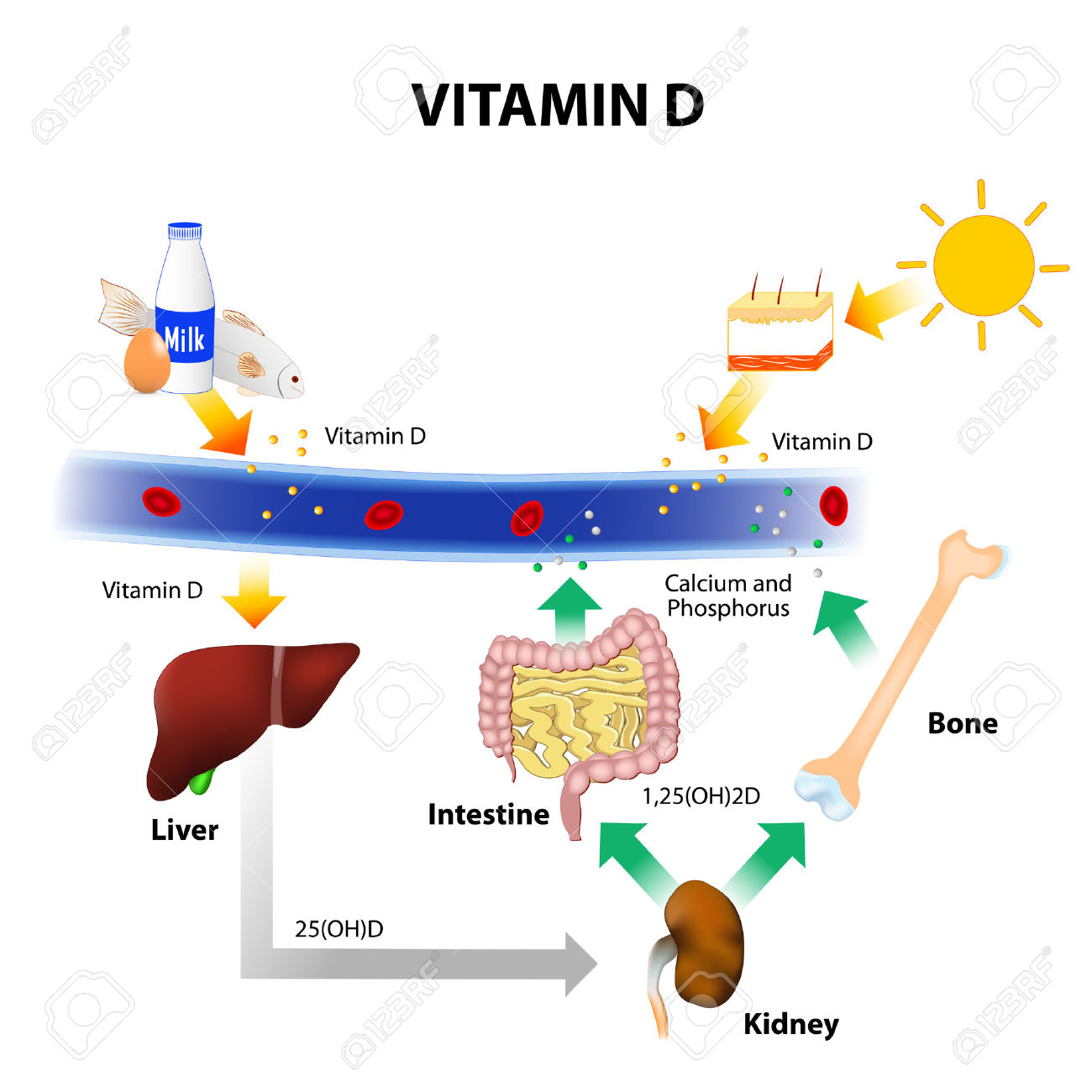
Vitamine D wordt vooral aangemaakt door zonlicht maar zit ook in bepaalde voeding. Hier een grafiek over vitamine D bronnen en hun werkzaamheid: (Tekst gaat verder onder grafiek)
Patiënten in de groep met hoge doses kregen 2 weken een dosis vitamine D3 van 8000 IE / dagelijks , gevolgd door 4000 IE / dagelijks. Patiënten in de lage dosis groep kregen een standaard vitamine D3 dosis van 400 IE / dagelijks.
Deze studie was een van de hoogtepunten op ASCO 2017 en er zal snel een fase III studie worden gepland. In tegenstelling tot medicijnen enz. hoeft u als patiënt natuurlijk niet te wachten op deze studie want overal kan vitamine D3 worden gekocht. Doe dat wel onder begeleiding van een goed gekwalificeerd orthomoleculair arts of natuurarts. En koop de goede opneembare vitamine D3. Zie ook onze lijsten, waaronder de darmkankerlijst.
Het abstract van de studie: SUNSHINE Study: Randomized double-blind phase II trial of vitamin D supplementation in patients with previously untreated metastatic colorectal cancer staat hieronder.
A high dose of vitamin D supplementation significantly improved progression-free survival (PFS) by about 2 months compared to a low dose for metastized colorectal cancer
SUNSHINE: Randomized double-blind phase II trial of vitamin D supplementation in patients with previously untreated metastatic colorectal cancer.
Sub-category:
Advanced Disease
Category:
Gastrointestinal (Colorectal) Cancer
Meeting:
2017 ASCO Annual Meeting
Abstract No:
3506
Citation:
J Clin Oncol 35, 2017 (suppl; abstr 3506)
Author(s): Kimmie Ng, Halla Sayed Nimeiri, Nadine Jackson McCleary, Thomas Adam Abrams, Matthew B. Yurgelun, James M. Cleary, Douglas Adam Rubinson, Deborah Schrag, Jill N. Allen, Dan Sayam Zuckerman, Rebecca A. Miksad, Emily Chan, Michael Constantine, Douglas Weckstein, Meredith Gail Faggen, Christian A. Thomas, Chryssanthi S. Kournioti, Christopher Mackintosh, Hui Zheng, Charles S. Fuchs; Dana-Farber Cancer Institute, Boston, MA; Robert H. Lurie Cancer Center of Northwestern University, Chicago, IL; Massachusetts General Hospital, Boston, MA; St. Luke's Mountain States Tumor Institute, Boise, ID; Beth Israel Deaconess Medical Center, Boston, MA; Vanderbilt University Medical Center, Nashville, TN; Dana-Farber Cancer Institute, Milford, MA; New Hampshire Oncology-Hematology PA, Hooksett, NH; Dana-Farber Cancer Institute, South Weymouth, MA; New England Cancer Specialists, Scarborough, ME; Yale New Haven Hospital, Boston, MA; Dana-Farber Cancer Institute/Partners CancerCare, Boston, MA
Background: In prospective observational studies of mCRC patients, higher plasma levels of 25-hydroxyvitamin D have been associated with improved progression-free (PFS) and overall survival (OS), but the role of vitamin D supplementation in the treatment of mCRC is unknown.
Methods: SUNSHINE was a multi-center double-blind phase II randomized controlled trial in previously untreated mCRC patients. Patients were eligible if they had histologically confirmed mCRC, no prior therapy for metastatic disease, ECOG PS 0-1, and were not taking vitamin D >2,000 IU/day x 1 year. All subjects received standard treatment with mFOLFOX6 + bevacizumab with 1:1 randomization to concurrent: HiVitD (vitamin D3 po 8,000 IU/d x 2 wks as loading dose followed by 4,000 IU/d) or LowVitD (standard vitamin D3 400 IU/d) until disease progression, intolerable toxicity, or withdrawal of consent. The primary endpoint was PFS, with the sample size designed to provide 80% power to detect a HR of 0.66 for PFS at a 1-sided alpha=0.2.
Results: From April 2012 to November 2016, 139 patients were randomized. Median age was 54 yrs (range 24-82), 57% were male, 77% were white, and 7% had received prior adjuvant chemo. Baseline characteristics were balanced between arms except ECOG PS = 0 was 42% vs. 60% in HiVitD vs. LowVitD. Median follow-up was 16.1 mos (range 0-45.9) and median compliance with VitD capsules was 98%. Patients randomized to HiVitD experienced longer PFS than those receiving LowVitD (median PFS, 12.4 vs. 10.7 mos, respectively; log rank P=0.03). After multivariate adjustment for prognostic variables, HR was 0.66 (95% CI, 0.45-0.99, 2-sided P=0.04). Comparing HiVitD vs LowVitD, RR was 58% vs. 63% (P=0.54) and disease control rate was 100% vs. 94% (P=0.05). The most common grade 3-4 toxicities were as expected for FOLFOX-bevacizumab, and none were related to vitamin D. Currently, 14 patients are still actively receiving treatment, and OS data are not yet mature.
Conclusion: SUNSHINE met its prespecified primary endpoint, with patients randomized to HiVitD experiencing longer PFS compared to those randomized to LowVitD. A larger confirmatory phase III randomized trial appears warranted. Clinical trial information: NCT01516216
Gerelateerde artikelen
- Hoge dosis vitamine D aanvullend op standaard chemo bij patienten met onbehandelde uitgezaaide darmkanker geeft klein voordeel in vergelijking met aanvullend normale dosis vitamine D
- Vitamine D-suppletie reguleert postoperatieve bloedwaarden van PD-L1 bij patiënten met spijsverteringskanker en verbetert sterk de overall overleving van patienten met de hoogste PD-L1 waarden copy 1
- Hoge dosis vitamine D3 naast chemo bij darmkanker geeft langere ziekteprogressie vrije tijd en betere controle van de ziekte dan lage dosis vitamine D3 en vermindert ook sterk de bijwerkingen van de chemo mFOLFOX6
- ATRA - all-trans-retinoic-acid - retinionezuur voorkomt en vermindert sterk de tumorgroei bij darmkanker blijkt uit dierstudies en darmflora van darmkankerpatienten copy 1
- Voedingssupplement met 6 voedingstoffen - MP 6 aanvullend op FOLFOX geeft langere progressievrije ziekte en minder ernstige bijwerkingen bij uitgezaaide gevorderde darmkanker.
- Vitamine D (25-hydroxyvitamin D) zorgt voor significant minder risico - tot wel 39 procent - op overlijden aan darmkanker
- Vitamine D (zonlicht/levertraan/vette vis) - circulerende vitamine D waarden spelen belangrijke rol in preventie van dikke darmkanker.
- Menatetrenone - analoog aan vitamine K2 - vermindert bij operabele leverkanker de kans op een recidief significant - 42,7 procent na 1 jaar en 27,3 procent na 3 jaar ) en verbetert 3 jaars overleving met 23 procent.
- Vitamine E en C voorkomt en geneest ontstekingen bij radiotherapie - bestraling bij dikke darmkanker.
- Antioxidanten - voedingsuppletie: calcium en meerdere soorten vitaminen hebben positief effect op een behandeling en ter voorkoming van recidief van darmkanker
Plaats een reactie ...
Reageer op "Hoge dosis vitamine D3 naast chemo bij darmkanker geeft langere ziekteprogressie vrije tijd en betere controle van de ziekte dan lage dosis vitamine D3 en vermindert ook sterk de bijwerkingen van de chemo mFOLFOX6"