

29 juli 2019: Lees ook dit artikel: hyperthermie-van-het-bekkengebied-naast-chemo-en-bestraling-en-daarna-operatie-verbetert-de-5-jaars-overall-overleving-met-23-procent-vs-chemo-en-bestraling-en-42-procent-vs-alleen-bestralen.html
11 februari 2018: Bron ASCO GU 2018
Aanvullend op onderstaande informatie is op ASCO 2018 de resultaten van een 11 jarige studie gepresenteerd waarin wordt bevestigd dat Radiofrequency-Induced Thermochemotherapy (hyperthermie met het Synergo systeem) een betere aanpak is van niet-spier invasieve blaaskanker met hoog risico dan BCG plus cystectomy in het voorkomen van een recidief met veel betere kwaliteit van leven omdat een volledige cystectomy (blaasverwijdering) niet nodig was en 80,6 procent van de patienten hun blaas konden behouden. Deze vorm van hyperthermie met het Synergo systeem wordt ook in Nederland toegepast o.a. in de Radboud in Nijmegen. (Zie ook dit PDF document over blaaskanker ) en mogelijke opties van behandelen. (tekst gaat verder onder plaatje van Synergo systeem)
Er is nog geen studierapport gepubliceerd maar hier de resultaten uit een presentatie tijdens ASCO GU 2018.
Dit studierapport: Intravesical radiofrequency-induced hyperthermia combined with chemotherapy for non-muscle-invasive bladder cancer is een publicatie uit 2015 van dezelfde studie en wel volledig te lezen of downloaden.
Dit zijn de nieuwe resultaten. (onderaan artikel een abstract met referentielijst):
A total of 67 patients (4 female, 63 male) have been enrolled, 65.7% of whom harbor carcinoma in situ. Alternatively, 85% of patients were treated with primary radiofrequency-induced thermochemotherapy effect. Bacillus Calmette-Guerin failed in 15%.
In 14.9% (10 of 67 patients), the tumor persisted at week 11 after induction therapy (proven by transurethral resection of bladder tumor). This persistence led to early cystectomy in 4 of 10 patients. Mean recurrence-free survival was 3.5 years. In cases of recurrence, 10.4% progressed to non–muscle-invasive bladder cancer, including 6% of metastatic tumors.
High-risk non–muscle-invasive bladder cancer was observed in 6% of patients, and led to cystectomy. Recurrence of non–muscle-invasive bladder cancer occurred in 1.5% of cases, with organ preservation.
The mortality rate was 1 in every 67 patients. Serious adverse events of radiofrequency-induced thermochemotherapy effect led to discontinuation in 9% of cases. The bladder preservation rate was 80.6%, with 53.8% (14 of 26 patients) achieving long-term efficacy for over 5 years.
Dr. Kilb concluded that radiofrequency-induced thermochemotherapy effect proved powerful in its ability to cure and maintain recurrence-free bladder cancer status in high-risk non–muscle-invasive bladder cancer in both the short and long term.
Risk of cystectomy was very low and risk of systemic progression leading to death from bladder cancer was minimal. Organ preservation was achieved in 80.6% of cases and lasted up to 11 years.
Radiofrequency-induced thermochemotherapy effect was shown to be an alternative to bacillus Calmette-Guerin and preferable to early cystectomy in high-risk non–muscle-invasive bladder cancer.
“After 10 years of follow-up,” Dr. Kilb noted, “we can confirm positive long-term results in terms of organ preservation and risk of progression. We hope to establish the Synergo system as an accepted therapy for high-risk non–muscle-invasive bladder cancer, included in guidelines for bladder cancer treatment. The system provides a more successful therapy for patients with high-risk non–muscle-invasive bladder cancer.”
update 12 maart 2010:
We hebben het abstract van deze studie er nu ook bijgeplaatst. Direct onder de introductietekst van 31 oktober 2009
Update 31 oktober 2009: Bron: website van Medical Enterprise.
Op verzoek van een woordvoerder van Medical Enterprise plaatsen we onderstaande informatie. Deze informatie is voor verantwoording van Medical Enterprise en we wijzen u op onze disclaimer. Medical-enterprises biedt aan blaaskankerpatiënten, voor oppervlakkige blaaskanker een combinatiebehandeling hyperthermie en Mitomycine C na operatieve verwijdering van zoveel mogelijk tumorweefsel. En met hoogsignificant positieve resultaten. Hier een stukje introductie gekopieerd van de website van Medical Enterprise en een deepliink naar deze website waarop ook adressen staan van de ziekenhuizen in Nederland en België (heel Europa) waar deze combinatiebehandeling wordt gegeven.
Bron: website van Medical Enterprise.
De arts bepaalt het type van behandeling of de combinatie van behandelingen aan op basis van de gegevens over de tumor(en) en de toestand van de patiënt. Indien er verscheidene behandelingsopties zijn, overleggen de arts en de patiënt samen over de beslissing. Synergo® In weerwil van de courant gebruikte behandelingen is het percentage van herhalingen van de tumor of vordering van de ziekte bij patiënten met middelhoog tot hoog risico groot.
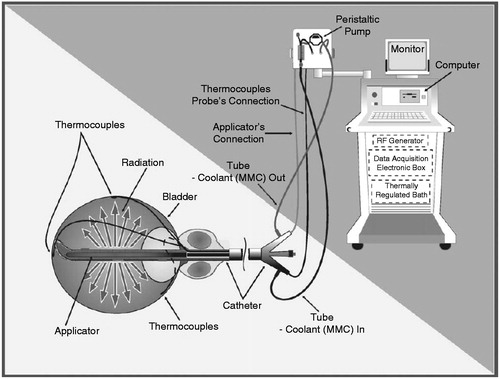
De technologie van Synergo combineert een plaatselijke verwarming van de blaaswand (hyperthermie) met het gelijktijdig spoelen van de urineblaas met een chemotherapeutisch geneesmiddel. Zowel de verwarming als het spoelen gebeuren door middel van een via de urethra in de urineblaas ingebrachte catheter De Synergo-catheter heeft drie belangrijke functies: 1. Gelijkmatige verwarming van de blaaswand door middel van een kleine antenne die radiostraling afgeeft (microgolven) 2. Controle van de temperatuur door middel van gevoelige thermokoppels, op verscheidene punten van de blaaswand. 3. Circulatie van het gekoelde chemotherapeutische geneesmiddel in en uit de blaas.
Zie website voor mooie verduidelijkende foto's. Alle gegevens worden door de Synergo-computer verwerkt en opgevolgd, zodat de blaastemperatuur tijdens de behandeling constant en stabiel blijft. De technologie van Synergo is goedgekeurd door de Europese normerende overheden ( CE normering ), terwijl de procedure voor goedkeuring door de U.S. Food and Drug Administration (FDA) loopt. De technologie is met succes toegepast in toonaangevende medische centra in diverse landen (Italië, Duitsland, Frankrijk, Oostenrijk, Israël en Nederland). Tot nu toe zijn honderden patiënten behandeld en hebben de behandelingen indrukwekkende resultaten opgeleverd. De behandeling van Synergo leidt tot een daling van de frequentie van de post-operatieve herhaling van tumoren (een vermindering van 58% naar 17% tijdens een opvolgingsperiode van twee jaar, en van 65% naar 26% in een geschatte opvolgingsperiode van vijf jaar), vergeleken met de tot nu toe courant toegepaste behandelingen.
De behandeling met Synergo omvat twee benaderingen: a. Behandeling voor de preventie van de herhaling van de tumor (profylaxe). Ze is bedoeld voor patiënten bij wie de tumor chirurgisch (TURT) of met laserstralen (TUF) is verwijderd. Deze behandeling is een alternatief voor het chemotherapeutisch spoelen van de urineblaas (zonder warmte) of de biologisch actieve (immunologische) behandelingen die vandaag courant worden gebruikt b. Behandeling voor de verwijdering van de tumor (ablatie). Ze is bedoeld voor patiënten met een sterk ontwikkelde tumor of uitgebreide kwaadaardige zones in de urineblaas (die moeilijk in één operatie te verwijderen zijn) en voor patiënten met vaak herhalende tumoren. Ze is ook bedoeld voor patiënten van wie de toestand geen verdoving mogelijk maakt. In beide gevallen wordt de patient met een serie van wekelijkse sessies van een uur ( profylactische patienten krijgen na de serie wekelijkse behandelingen nog een aantal maandelijkse behandelingen ) op de polikliniek behandeld. Na elke behandeling kan de patiënt zijn gewone dagelijkse bezigheden of werkzaamheden hervatten. De veiligheid van de technologie van Synergo is in een reeks klinische studies onderzocht en bewezen. De bijwerkingen van de behandelingen zijn meestal licht en tijdelijk (plaatselijke pijn, brandend gevoel tijdens het urineren, drang en frequentie van het urineren) en verdwijnen meestal binnen de 48-72 uren na de behandeling; ze houden geen gevaar in voor de patiënt. Opvolging van de patiënt Na de behandeling voor kanker van de urineblaas blijft men de patiënt zorgvuldig medisch opvolgen met regelmatige cystoscopieën en andere tests, afhankelijk van het geval. Dit is nodig om een eventuele terugkeer van de ziekte zo snel mogelijk op te sporen. Eerst is de frequentie van de controles hoog (om de drie maanden), later worden ze meer gespreid, volgens het oordeel van de arts. De opvolgingsbezoeken zijn erg belangrijk en de patiënten moeten hun best doen om het aanbevolen opvolgingsschema te volgen.
J Urol. 2009 Oct;182(4):1313-7. Epub 2009 Aug 14.
Combined thermo-chemotherapy for recurrent bladder cancer after bacillus Calmette-Guerin.
Nativ O, Witjes JA, Hendricksen K, Cohen M, Kedar D, Sidi A, Colombo R, Leibovitch I.
Urology Department, Bnai-Zion Medical Center, Haifa, Israel. ofer.nativ@b-zion.org.il
Comment in:
PURPOSE: Despite an initial adequate response many patients with nonmuscle invasive urothelial cell carcinoma of the bladder eventually have recurrence after intravesical bacillus Calmette-Guerin treatments. We evaluated the efficacy of combined bladder wall hyperthermia and intravesical mitomycin C instillation (thermo-chemotherapy) in cases of recurrence after bacillus Calmette-Guerin.
MATERIALS AND METHODS: A total of 111 patients with recurrent papillary nonmuscle invasive urothelial cell carcinoma of the bladder after previous bacillus Calmette-Guerin treatment underwent complete bladder tumor resection and were referred for prophylactic adjuvant treatment with thermo-chemotherapy. Treatment was received on an outpatient basis weekly for 6 weeks, followed by 6 maintenance sessions at 4 to 6-week intervals. Each treatment included 2, 30-minute cycles of 20 mg mitomycin C and bladder wall hyperthermia to 42C +/- 2C. Cystoscopy and urine cytology were performed after the completion of induction treatment and every 3 months thereafter.
RESULTS: The Kaplan-Meier estimated disease-free survival rate was 85% and 56% after 1 and 2 years, respectively. No maintenance treatment was associated with decreased efficacy, that is the recurrence rate was 61% at 2 years vs 39% in those with maintenance treatments (p = 0.01). The progression rate was 3%.
CONCLUSIONS: Thermo-chemotherapy may be effective for papillary nonmuscle invasive urothelial cell carcinoma of the bladder that recurs after BCG treatment without increasing the risk of tumor progression. Maintenance therapy is important and improves the outcome.
PMID: 19683278 [PubMed - indexed for MEDLINE]
Meest recente publicaties van hyperthermie en chemo bij blaaskanker zijn deze, maar op website van Medical Enterprise en in Pubmed zijn veel meer studies te vinden over hyperthermie als aanvulling op chemo en blaaskanker:
1. Van der Heijden A.G, Cornelius F. J. J, Verhaegh G, O'Donnell M.A, Schalken J.A, Witjes J.A. The Effect of Hyperthermia on Mitomycin-C Induced Cytotoxicity in Four Human Bladder Cancer Cell Lines. Submitted for publication to J Urol 2004.
2. Van der Heijden A.G, Kiemeney L.A, Gofrit O.N, Nativ O, Sidi A, Leib Z, Colombo R, Naspro R, Pavone M, Baniel J, Hasner F, Witjes J.A. Preliminary European Results of Local Microwave Hyperthermia and Chemotherapy Treatment in Intermediate or High Risk Superficial Transitional Cell Carcinoma of the Bladder. Accepted for publication in Eur Urol: 2004.
3. Gofrit O.N, Shapiro A, Pode D, Sidi A, Nativ O, Leib Z, Witjes J.A, Van Der Heijden A.G, Naspro R, Colombo R. Combined Local Bladder Hyperthermia and Intravesical Chemotherapy for the Treatment of High Grade Superficial Bladder Cancer. Urol 63(3):466-471;2004.
Radiofrequency-induced thermochemotherapy effect was shown to be an alternative to bacillus Calmette-Guerin and preferable to early cystectomy in high-risk non–muscle-invasive bladder cancer.
Intravesical radiofrequency-induced hyperthermia combined with chemotherapy for non-muscle-invasive bladder cancer
Abstract
Although many treatment modalities and schedules for non-muscle-invasive bladder cancer (NMIBC) exist, all yet prove to have limitations. Therefore the search for new forms of therapy continues. One of these forms consists of combining intravesical chemotherapy, typically mitomycin C (MMC), with hyperthermia achieved by a microwave-applicator. We aimed to review the current status of intravesical radiofrequency (RF) induced chemohyperthermia (CHT) for NMIBC with regard to efficacy, adverse-events (AEs) and its future perspective. A search for RF-induced CHT in MEDLINE, Embase, Cochrane and ClinicalTrials.gov databases was performed. Relevant conference abstracts were searched for manually. If applicable, experts on the area were consulted. Papers were selected based on abstract and title. A table of newly published clinical trials since 2011 was constructed. No meta-analysis could be performed based on these new papers. Efficacy proved to be better for RF-induced CHT compared to both MMC alone and bacillus Calmette–Guérin (BCG) instillations, with the latter being based on just one abstract of a randomised controlled trial. The AE rate in CHT is higher compared to MMC instillation, but is similar compared to BCG, albeit different in the type of AE. In almost all studies no severe AEs are reported. Although heterogeneity in methodology exists, RF-induced CHT seems promising. However, alternative methods of applying hyperthermia are starting to present their first results, imposing as effective options too. Intravesical RF-induced CHT may become an alternative for BCG instillation, and possibly for cystectomy, although further level 1 evidence is required for both reliable and reproducible data on efficacy and adverse events.
Conclusion
Radiofrequency-induced chemo-hyperthermia remains a promising treatment modality which appears to be a potential alternative to BCG immunotherapy. It can also be used in patients unfit to undergo radical cystectomy, or to prolong bladder preservation time. Adverse events and safety profile seem to be acceptable in the context of the indication for RF-induced CHT. Nonetheless, a more solid scientific basis is needed to define the position of RF-induced CHT in relation to other hyperthermic treatment modalities and in relation to the newly emerged non-hyperthermia treatments.
Declaration of interest
J.A.W. is an investigator for Medical Enterprise Ltd (MEL), Amsterdam, without financial compensation and no conflict of interest, and was an adviser for MEL Amsterdam in 2014, with financial compensation and no conflict of interest. The other authors have no other interests to declare. The authors alone are responsible for the content and writing of the paper.
References
- Babjuk M, Böhle A, Burger M, Compérat E, Kaasinen E, Palou J, et al. Guidelines on non-muscle-invasive bladder cancer (Ta, T1 and CIS). Eur Urol 2015. http://uroweb.org/wp-content/uploads/EAU-Guidelines-Non-muscle-invasive-Bladder-Cancer-2015-v1.pdf
- Sylvester RJ, van der Meijden AP, Oosterlinck W, Witjes JA, Bouffioux C, Denis L, et al. Predicting recurrence and progression in individual patients with stage Ta T1 bladder cancer using EORTC risk tables: A combined analysis of 2596 patients from seven EORTC trials. Eur Urol 2006;49:466–75; discussion 475–7 ,
- Fernandez-Gomez J, Madero R, Solsona E, Unda M, Martinez-Pineiro L, Ojea A, et al. The EORTC tables overestimate the risk of recurrence and progression in patients with non-muscle-invasive bladder cancer treated with bacillus Calmette–Guerin: External validation of the EORTC risk tables. Eur Urol 2011;60:423–30 ,
- Slater SE, Patel P, Viney R, Foster M, Porfiri E, James ND, et al. The effects and effectiveness of electromotive drug administration and chemohyperthermia for treating non-muscle invasive bladder cancer. Ann R Coll Surg Engl 2014;96:415–19 ,
- England HR, Anderson JD, Minasian H, Marshall VR, Molland EA, Blandy JP. The therapeutic application of hyperthermia in the bladder. Br J Urol 1975;47:849–52 ,
- Soria F, Milla P, Fiorito C, Pisano F, Sogni F, Di Marco M, et al. Efficacy and safety of a new device for intravesical thermochemotherapy in non-grade 3 BCG recurrent NMIBC: A phase I–II study. World J Urol 2015. doi: 10.1007/s00345-015-1595-3. Epub 2015 May 31 ,
- Sousa A, Inman BA, Pineiro I, Monserrat V, Perez A, Aparici V, et al. A clinical trial of neoadjuvant hyperthermic intravesical chemotherapy (HIVEC) for treating intermediate and high-risk non-muscle invasive bladder cancer. Int J Hyperthermia 2014;30:166–70 ,
- Oliveira TR, Stauffer PR, Lee CT, Landon CD, Etienne W, Ashcraft KA, et al. Magnetic fluid hyperthermia for bladder cancer: A preclinical dosimetry study. Int J Hyperthermia 2013;29:835–44 ,
- Inman BA, Stauffer PR, Craciunescu OA, Maccarini PF, Dewhirst MW, Vujaskovic Z. A pilot clinical trial of intravesical mitomycin-C and external deep pelvic hyperthermia for non-muscle-invasive bladder cancer. Int J Hyperthermia 2014;30:171–5 ,
- Colombo R, Lev A, Da Pozzo LF, Freschi M, Gallus G, Rigatti P. A new approach using local combined microwave hyperthermia and chemotherapy in superficial transitional bladder carcinoma treatment. J Urol 1995;153:959–63 ,
- Lammers RJ, Witjes JA, Inman BA, Leibovitch I, Laufer M, Nativ O, et al. The role of a combined regimen with intravesical chemotherapy and hyperthermia in the management of non-muscle-invasive bladder cancer: A systematic review. Eur Urol 2011;60:81–93 ,
- Mazzoleni F, Albo G, Verweij F, Botteri E, Detti S, Colombo R, et al. Thermo-chemotherapy for superficial transitional cell carcinoma of the bladder. Results of a multicentric clinical study: ‘Synergo lombardia’. Anticancer Res 2010;30:1538–9 ,
- Paroni R, Salonia A, Lev A, Da Pozzo LF, Cighetti G, Montorsi F, et al. Effect of local hyperthermia of the bladder on mitomycin C pharmacokinetics during intravesical chemotherapy for the treatment of superficial transitional cell carcinoma. Br J Clin Pharmacol 2001;52:273–8 ,
- Haveman J, Smals OA, Rodermond HM. Effects of hyperthermia on the rat bladder: A pre-clinical study on thermometry and functional damage after treatment. Int J Hyperthermia 2003;19:45–57 ,
- Matzkin H, Rangel MC, Soloway MS. In vitro study of the effect of hyperthermia on normal bladder cell line and on five different transitional cell carcinoma cell lines. J Urol 1992;147:1671–4 ,
- van der Heijden AG, Hulsbergen-Van de Kaa CA, Witjes JA. The influence of thermo-chemotherapy on bladder tumours: An immunohistochemical analysis. World J Urol 2007;25:303–8 ,
- van der Heijden AG, Verhaegh G, Jansen CF, Schalken JA, Witjes JA. Effect of hyperthermia on the cytotoxicity of 4 chemotherapeutic agents currently used for the treatment of transitional cell carcinoma of the bladder: An in vitro study. J Urol 2005;173:1375–80 ,
- Uchibayashi T, Lee SW, Kunimi K, Ohkawa M, Endo Y, Noguchi M, et al. Studies of effects of anticancer agents in combination with/without hyperthermia on metastasized human bladder cancer cells in chick embryos using the polymerase chain reaction technique. Cancer Chemother Pharmacol 1994;35:S84–7 ,
- Arends TJ, Falke J, Lammers RJ, Somford DM, Hendriks JC, de Weijert MC, et al. Urinary cytokines in patients treated with intravesical mitomycin-C with and without hyperthermia. World J Urol 2015;33:1411–17 ,
- Colombo R, Da Pozzo LF, Lev A, Freschi M, Gallus G, Rigatti P. Neoadjuvant combined microwave induced local hyperthermia and topical chemotherapy vs. chemotherapy alone for superficial bladder cancer. J Urol 1996;155:1227–32 ,
- Colombo R, Salonia A, Da Pozzo LF, Naspro R, Freschi M, Paroni R, et al. Combination of intravesical chemotherapy and hyperthermia for the treatment of superficial bladder cancer: Preliminary clinical experience. Crit Rev Oncol Hematol 2003;47:127–39 ,
- Farr S, Chess-Williams R, McDermott C. Selective cytotoxicity of gemcitabine on superficial malignant vs normal human urothelial cells and the effects of hyperthermia. Asia Pac J Clin Oncol 2014;10:131 ,
- Mauroy B, Bonnal JL, Prevost B, Chive M, Lhotellier V, Sozanski JP, et al. Etude de la synergie hyperthermie micro-onde/chimiotherapie intravesicale dans la prevention des recidives des tumeurs superficielles de vessie. [Study of the synergy of microwave hyperthermia/intravesical chemotherapy in the prevention of recurrences of superficial tumours of the bladder]. Prog Urol 1999;9:69–80 ,
- Wallner KE, Banda M, Li GC. Hyperthermic enhancement of cell killing by mitomycin C in mitomycin C-resistant Chinese hamster ovary cells. Cancer Res 1987;47:1308–12 ,
- Moskovitz B, Halachmi S, Moskovitz M, Nativ O, Nativ O. 10-year single-center experience of combined intravesical chemohyperthermia for nonmuscle invasive bladder cancer. Future Oncol 2012;8:1041–9 ,
- Volpe A, Racioppi M, Bongiovanni L, D’Agostino D, Totaro A, D’Addessi A, et al. Thermochemotherapy for non-muscle-invasive bladder cancer: Is there a chance to avoid early cystectomy? Urol Int 2012;89:311–18 ,
- Maffezzini M, Campodonico F, Canepa G, Manuputty EE, Tamagno S, Puntoni M. Intravesical mitomycin C combined with local microwave hyperthermia in non-muscle-invasive bladder cancer with increased European Organization for Research and Treatment of Cancer (EORTC) score risk of recurrence and progression. Cancer Chemother Pharmacol 2014;73:925–30 ,
- Arends TJ, van der Heijden AG, Witjes JA. Combined chemohyperthermia: 10-year single center experience in 160 patients with nonmuscle invasive bladder cancer. J Urol 2014;192:708–13 ,
- Kiss B, Schneider S, Thalmann GN, Roth B. Is thermochemotherapy with the Synergo system a viable treatment option in patients with recurrent non-muscle-invasive bladder cancer? Int J Urol 2015;22:158–62 ,
- Sooriakumaran P, Chiocchia V, Dutton S, Pai A, Ayres BE, Le Roux P, et al. Predictive factors for time to progression after hyperthermic mitomycin C treatment for high-risk non-muscle invasive urothelial carcinoma of the bladder: An observational cohort study of 97 patients. Urol Int 2015. doi: 10.1159/000435788. Epub 2015 Aug 6 ,
- Lüdecke G, Hasner F, Hanitzsch H, Schmidt M. The German study group of intravesical hyperthermia-chemotherapy in non-muscle-invasive bladder cancer presents their long-term results in efficacy and tolerability for optimized adjuvant therapy and bladder preservation. J Clin Oncol 2013;31:S ,
- Lüdecke G, Shchafer L, Nativ O, Witzsch U, Hanitzsch H, Hasner F, et al. Radiofrequence induced hyperthermia chemotherapy (RIHTC) in high-risk non-muscle invasive bladder cancer (NMIBC): Multiinstitutional, international outcome analysis of 271 treated patients with a follow-up time of more than 2 years. Eur Urol 2015;14:e949 ,
- Arends TJH, Nativ O, Maffezzini M, De Cobelli O, Van Der Heijden AG, Witjes JA. Results of the first randomized controlled trial comparing intravesical radiofrequency induced chemohyperthermia with mitomycin-C vs. BCG for adjuvant treatment of patients with intermediate-and high-risk non-muscle invasive bladder cancer. Eur Urol 2015;14:e944 ,
- Colombo R, Da Pozzo LF, Lev A, Salonia A, Rigatti P, Leib Z, et al. Local microwave hyperthermia and intravesical chemotherapy as bladder sparing treatment for select multifocal and unresectable superficial bladder tumors. J Urol 1998;159:783–7 ,
- Rigatti P, Lev A, Colombo R. Combined intravesical chemotherapy with mitomycin C and local bladder microwave-induced hyperthermia as a preoperative therapy for superficial bladder tumors. A preliminary clinical study. Eur Urol 1991;20:204–10 ,
- van der Heijden AG, Kiemeney LA, Gofrit ON, Nativ O, Sidi A, Leib Z, et al. Preliminary European results of local microwave hyperthermia and chemotherapy treatment in intermediate or high risk superficial transitional cell carcinoma of the bladder. Eur Urol 2004;46:65–71; discussion: 72 ,
- Witjes AJ, Hendricksen K, Gofrit O, Risi O, Nativ O. Intravesical hyperthermia and mitomycin-C for carcinoma in situ of the urinary bladder: Experience of the European Synergo working party. World J Urol 2009;27:319–24 ,
- Halachmi S, Moskovitz B, Maffezzini M, Conti G, Verweij F, Kedar D, et al. Intravesical mitomycin C combined with hyperthermia for patients with T1G3 transitional cell carcinoma of the bladder. Urol Oncol 2011;29:259–64 ,
- Ayres BE, Connor A, Corbishley C, Bailey MJ. Radiofrequency hyperthermia and mitomcin C for the management of frail patients with high-risk non-muscle invasive bladder cancer who fail intravesical BCG treatment. BJU Int 2010;106:8 ,
- Colombo R, Brausi M, Da Pozzo L, Salonia A, Montorsi F, Scattoni V, et al. Thermo-chemotherapy and electromotive drug administration of mitomycin C in superficial bladder cancer eradication. a pilot study on marker lesion. Eur Urol 2001;39:95–100 ,
- Colombo R, Salonia A, Leib Z, Pavone-Macaluso M, Engelstein D. Long-term outcomes of a randomized controlled trial comparing thermochemotherapy with mitomycin-C alone as adjuvant treatment for non-muscle-invasive bladder cancer (NMIBC). BJU Int 2011;107:912–18 ,
- Kelly JD, Buckley L, Devall AJ, Loubière LS, Barnwell JM, Feneley MR, et al. HYMN: a randomised controlled phase III trial comparing hyperthermia plus mitomycin to a second course of bacillus Calmette–Guerin (BCG) or institutional standard in patients with recurrence of non-muscle invasive bladder cancer (NMIBC) following induction or maintenance therapy. Manchester: BAUS meeting, 2015
- Ekin RG, Akarken I, Zorlu F, Tarhan H, Kucuk U, Yildirim Z, et al. Intravesical bacillus Calmette–Guerin vs. chemohyperthermia for high-risk non-muscle-invasive bladder cancer. Can Urol Assoc J 2015;9:E278–83 ,
- Nair R, Pai A, Kaul A, Ayres B, Bailey M, Perry M, et al. Challenging the gold standard: A comparison of long-term disease specific outcomes for high-risk non-muscle invasive bladder cancer treated with mitomycin hyperthermia and radical cystectomy. Eur Urol 2014;13:e1109 ,
- Rath-Wolfson L, Moskovitz B, Dekel Y, Kugel V, Koren R. Combined intravesical hyperthermia and mitomycin chemotherapy: A preliminary in vivo study. Int J Exp Pathol 2003;84:145–52 ,
- Hashimoto T, Hisazumi H, Nakajima K, Matsubara F. Studies on endocrine changes induced by 8 MHz local radiofrequency hyperthermia in patients with bladder cancer. Int J Hyperthermia 1991;7:551–7 ,
- Hasner F, Thueroff S, Chaussy C. Combined thermochemotherapy (Synergo) in non muscle invasive bladder cancer (NMIBC): 8 year follow up of a prospective monocentric cohort study. Urology 2009;74:S145 ,
- Ekin RG, Akarken I, Cakmak O, Tarhan H, Celik O, Ilbey YO, et al. Results of intravesical chemo-hyperthermia in high-risk non-muscle invasive bladder cancer. Asian Pac J Cancer Prev 2015;16:3241–5 ,
- Lüdecke GC, Schafer L, Weidner W, Hasner F, Hanitzsch H, Schmidt M. Organ preservation in high- and extreme high risk non-muscle-invasive bladder cancer (NMIBC): Outcome analysis of an interventional cohort study of the German Hyperthermia Chemotherapy Group in efficacy and side effects. Eur Urol 2013;12:e707–8 ,
Gerelateerde artikelen
- COMBAT systeem - hyperthermiespoelingen met mitomycine C bij blaaskankerpatienten wordt ook toegepast in Nederlandse academische ziekenhuizen en geeft goede resultaten in voorkomen van recidief.
- Hyperthermie van het bekkengebied naast chemo en bestraling en daarna operatie verbetert de 5-jaars overall overleving met 23 procent vs chemo en bestraling en 42 procent vs alleen bestralen.
- Hyperthermie bij blaaskanker: Chemo (mitomycin C) in combinatie met hyperthermie is significant effectiever dan chemo alleen ter voorkoming van recidief van blaaskanker na operatie en BCC.
- Hyperthermie plus chemo (mitomycine C) is aanzienlijk effectiever dan chemo alleen om een recidief te voorkomen van blaaskanker na operatie
- Hyperthermie naast bestraling en chemo na operatie bij blaaskankerpatienten (T1 en T2) met verhoogd risico op recidief geeft goede resultaten op overall overleving en ziektevrije tijd historisch vergeleken
- Lokale hyperthermie zorgt voor hoog significant betere resultaten bij blaaskankerpatiënten tegenover alleen chemo, aldus gerandomiseerde studie.
- Hyperthermie aanvullend of vooraf aan operatie of andere behandelingen bij blaaskanker, ook in gevorderd stadium is vaak succesvol.
Plaats een reactie ...
Reageer op "Hyperthermie bij blaaskanker: Chemo (mitomycin C) in combinatie met hyperthermie is significant effectiever dan chemo alleen ter voorkoming van recidief van blaaskanker na operatie en BCC."