

Mocht u kanker-actueel de moeite waard vinden en ons willen ondersteunen om kanker-actueel online te houden dan kunt u ons machtigen voor een periodieke donatie via donaties: https://kanker-actueel.nl/NL/donaties.html of doneer al of niet anoniem op - rekeningnummer NL79 RABO 0372931138 t.n.v. Stichting Gezondheid Actueel in Amersfoort. Onze IBANcode is NL79 RABO 0372 9311 38
Elk bedrag is welkom. En we zijn een ANBI instelling dus uw donatie of gift is in principe aftrekbaar voor de belasting.
En als donateur kunt u ook korting krijgen bij verschillende bedrijven:
14 maart 2016: Bron: Theranostics 2016 Feb 13;6(4):501-10. doi: 10.7150/thno.13702. eCollection 2016.
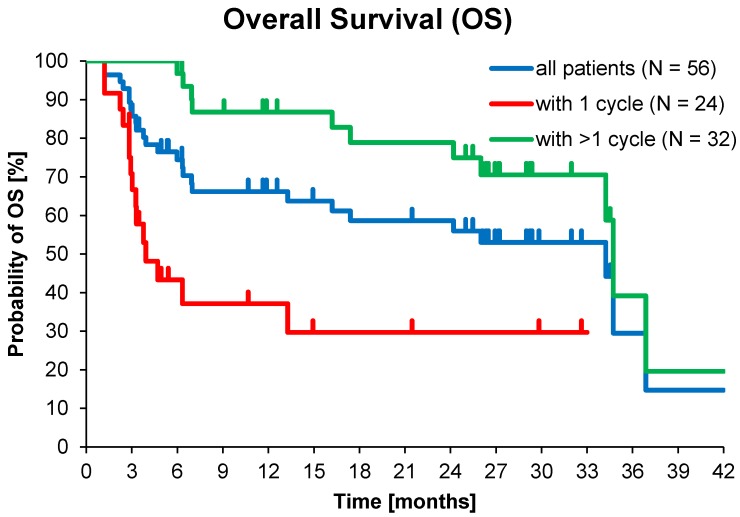
Wanneer het stofje 177Lu-Dotatate wordt toegevoegd aan de Peptide Receptor Radionuclide Therapie (PRRT) dan geeft deze behandeling 79 procent minder kans te overlijden aan tumoren van neuro endocrine afkomst ontstaan in de spijsverteringsorganen en spijsverteringskanalen, zo toont een langjarige fase III studie aan. Hieronder hebben we al eerder het succes van Peptide Receptor Radionuclide Therapie (PRRT) gemeld maar nu is ook het aanvullende studierapport met als toevoeging 177Lu-Dotatate gepubliceerd. Opvallend is dat wie meer dan 1 PRRT behandeling krijgt de mediane overall overleving enorm stijgt met enkele jaren verschil: (32.0 vs. 3.8 and 34.7 vs. 3.9 maanden)
Het volledige studierapport van deze studie: [(177)Lu-DOTA](0)-D-Phe(1)-Tyr(3)-Octreotide ((177)Lu-DOTATOC) For Peptide Receptor Radiotherapy in Patients with Advanced Neuroendocrine Tumours is gratis in te zien of te downloaden. Het abstract ervan staat onderaan artikel.
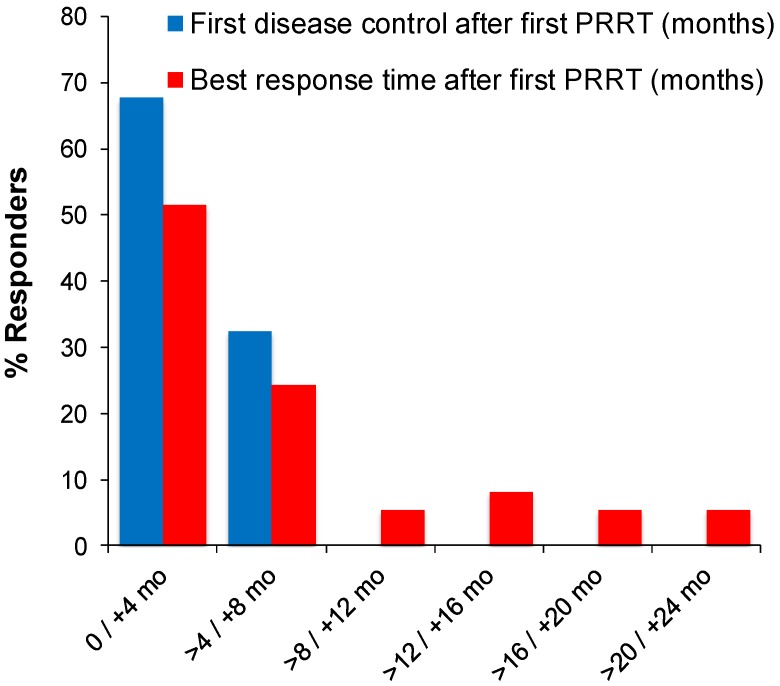
Mediane progressievrije tijd (PFS) en overall overleving (OS) waren statistisch significant veel beter voor patiënten die meerdere keren met PRRT waren behandeld >1 PRRT (32.0 vs. 3.8 en 34.7 vs. 3.9 maanden). Echter ook bij patiënten die controle over de ziekte kregen met 1 behandeling van PRRT met eenmalige toevoeging van 177Lu-DOTATOC cycle (mediane repons 29.2 %), werd een individuele progressievrije tijd tot soms 30 maanden gezien en individuele overall overleving van tot soms 33 maanden. daarmee bevesitgend dat directe toevoeging van 177Lu-Dotatate aan de PRRT behandeling wenselijk is.
Zie voor meer geegevens het studierapprot of abstract hieronder met referentieliijst.
Zoals eerder geschreven in Rotterdam is in het Erasmus Medisch Centrum een speciaal centrum voor PRRT.
29 september 2015: Bron: Europees oncologie congres in Wenen en Nu.nl
Peptide Receptor Radionuclide Therapie (PRRT) - inwendige bestraling met radioactieve geladen eiwitten bij patiënten met neuro-endocriene tumoren geeft uitstekende resultaten - 4 tot 6 jaar langerere overleving - in vergelijking met de standaard behandeling van radio-actief jodium. Uit de resultaten bljkt ook dat de behandeling bij 80 procent van de patiënten met neuro-endocriene tumoren aanslaat. De studieresultaten werden gepresenteerd op het Europese oncologie congres in Wenen.
De Peptide Receptor Radionuclide Therapie (PRRT) is in het Erasmus Medisch Centrum ontwikkeld onder leiding van prof. dr. Eric Krenning: 'Nieuw aan deze behandeling is dat kankercellen door het toedienen van kleine radioactieve eiwitten (peptiden) via een infuus inwendig worden bestraald. De kleine eiwitten hechten zich alleen aan de kankercellen en door de radioactieve straling worden de kankercellen vernietigd of wordt de groei ervan verminderd. Zo kunnen we de tumor zeer gericht en nog effectiever behandelen zonder gezond weefsel aan te tasten.' Ook andere vormen van kanker waaronder bv. prostaatkanker zouden met deze methode kunnen worden behandeld.
Het nieuwste studierapport is nog niet vrijgegeven maar een eerder studierapport verscheen in 2013: Treatment of Gastroenteropancreatic Neuroendocrine Tumors with Peptide Receptor Radionuclide Therapy waarbij PRRT werd toegepast bij endocreine tumoren in de alvleesklier
Foto: grafiek van OS bij PRRT bij alvleeskliertumoren
Een andere interessante studie is waarbij bepaalde receptorenexpressie voorspelt of de aanpak aan zal slaan of niet: Predictors of Long-Term Outcome in Patients with Well-Differentiated Gastroenteropancreatic Neuroendocrine Tumors After Peptide Receptor Radionuclide Therapy with 177Lu-Octreotate welke gratis is in te zien.
Op de website van het PRRT behandelcentrum van het Erasmus Medisch centrum staan nog meer publicaties:
Neuro-endocriene tumoren komen voor in de alvleesklier, darmen en longen en zijn vaak hormoongerelateerd. Deze tumoren zijn meestal langzaam groeiend en worden vaak pas in een laat stadium ontdekt als ze al door het hele lichaam zijn verspreid en dan met name in de alvleesklier, longen en darmen. Vaak is het dan te laat om de tumor geheel te laten verwijderen door een chirurgische ingreep.
Met de standaardbehandeling konden tumoren acht maanden effectief behandeld worden, nu kunnen tumoren vijf keer langer bestreden worden. Uit eerder onderzoek bleek al, dat met deze behandeling patiënten gemiddeld vier tot zes jaar langer leven dan met bestaande behandelingen én dat de kwaliteit van leven aanmerkelijk wordt verbeterd.
Ook blijkt dat de behandeling bij 80 procent van de patiënten met neuro-endocriene tumoren aanslaat. Nu de effectiviteit met deze resultaten is bewezen, wordt de nieuwe behandeling naar verwachting in 2016 geregistreerd door de Amerikaanse Food and Drug Administration (FDA) en het Europees geneesmiddelenbureau (EMA). Patiënten met neuro-endocriene tumoren kunnen dan met de therapie worden behandeld. Met deze registratie komt ook de behandeling van andere kankersoorten op korte termijn beschikbaar voor patiënten.
Ter vergelijking wat PRRT als meerwaarde heeft zie ook dit artikel:
A radiolabeled somatostatin analog compound, 177Lu-DOTA0-Tyr3-Octreotate (177Lu-Dotatate), reduced the risk of disease progression or death by 79% in the international phase III NETTER-1 population of previously treated, advanced neuroendocrine tumors of midgut origin
[(177)Lu-DOTA](0)-D-Phe(1)-Tyr(3)-Octreotide ((177)Lu-DOTATOC) For Peptide Receptor Radiotherapy in Patients with Advanced Neuroendocrine Tumours: A Phase-II Study.
Abstract
PURPOSE:
To characterise efficacy and safety of (177)Lu-DOTATOC as agent for peptide receptor radiotherapy (PRRT) of advanced neuroendocrine tumours (NET).
PATIENTS AND METHODS:
Fifty-six subjects with metastasized and progressive NET (50% gastroenteral, 26.8% pancreatic, 23.2% other primary sites) treated consecutively with (177)Lu-DOTATOC were analysed retrospectively. Subjects were administered (177)Lu-DOTATOC (mean 2.1 cycles; range 1-4) as 7.0GBq (median) doses at three-monthly intervals. Efficacy was analysed using CT and/or MRI according to RECIST 1.1 criteria and results were stratified for the number of administered cycles and the primary tumour origin.
RESULTS:
In the total NET population (A), median progression-free (PFS) and overall survival (OS) were 17.4 and 34.2 months, respectively, assessed in a follow-up time (mean ± SD) of 16.1 ± 12.4 months. In patients receiving more than one cycle, mean follow-up time was 22.4 ± 11.0 months for all NETs (B) and PFS was 32.0 months for all NETs (B), 34.5 months for GEP-NET (C), and 11.9 months for other NETs (D). Objective response rates (Complete/Partial Responses) were 33.9%, 40.6%, 54.2%, and 0% for A, B, C, and D groups, respectively, while disease control rates in the same were 66.1%, 93.8%, 100%, and 75%. Complete responses (16.1%, 18.8% and 25.0% for groups A, B and C) were high, 78% of which were maintained throughout the follow up. There were no serious adverse events. One case of self-limiting grade 3 myelotoxicity was reported. Although 20% of patients had mild renal insufficiency at baseline, there was no evidence of exacerbated or de novo renal toxicity after treatment.
CONCLUSION:
(177)Lu-DOTATOC is a novel agent for PRRT with major potential to induce objective tumour responses and sustained disease control in progressive neuroendocrine tumours, even when administered in moderate activities. The observed safety profile suggests a particularly favourable therapeutic index, including in patients with impaired bone marrow or renal function, which reflects a uniquely low uptake of (177)Lu-DOTATOC by normal organs.
References
Gerelateerde artikelen
- 177Lu-DOTATATE geeft uitstekende resultaten op overleving bij de behandeling van NET tumoren - neuro-endocriene tumoren. Vooral alvleesklier gerelateerde NET tumoren reageren zeer goed.
- 177Lu-edotreotide verbetert de progressievrije overleving ten opzichte van everolimus bij GEP-NET tumoren van graad 1 of 2 (neuro endocriene tumoren gerelateerd aan alvleesklierkanker en spijsverteringskanker)
- von Hippel–Lindau ziekte blijkt uitstekend te behandelen te zijn met Belzutifan en voorkomt verder ontwikkelen van neuro endocriene tumoren
- Immuuntherapie met pembrolizumab geeft weinig tot geen effect bij uitgezaaide neuro endocriene tumoren en andere aanpak lijkt noodzakelijk voor deze vorm van kanker
- CAPTEM een combinatie van Xeloda - capecitabine met temozolomide - temodal zorgt voor spectaculaire resultaten (97% minimaal stabiele ziekte) bij patiënten met alvleesklierkanker (NET3), carcinoid, schildkliertumoren en hypofyse tumoren
- Carcinoid Syndroom - Carcinoide tumoren informatie algemeen
- Everolimus plus octreotide (LAR) verbetert voor gevorderde neuro endocriene tumoren - carcinoidsyndroom - met een laag en gemiddeld stadium de progressievrije overlevingstijd
- Peptide Receptor Radionuclide Therapie (PRRT) geeft uitstekende resultaten - 4 tot 6 jaar langere overleving - bij patiënten met neuro endocriene tumoren
- Sandostatine LAR (langwerkend octreotide-acetaat). werkt uitstekend bij patiënten met Carcinoid Syndroom - Carcinoide tumoren, aldus studie uit Engeland, maar wordt ook in Rotterdam - Erasmus Medisch Centrum toegepast.
- Hoge dosis radioactief jodium - ook wel bekend als inwendige bestraling - als aanvulling gegeven aan patiënten met uitgezaaide carcinoid, waarbij alle andere medicijnen en aanpak niets hielp geeft significant betere resultaten op langere overlevingstijd
Plaats een reactie ...
Reageer op "Peptide Receptor Radionuclide Therapie (PRRT) geeft uitstekende resultaten - 4 tot 6 jaar langere overleving - bij patiënten met neuro endocriene tumoren"