

Mocht u kanker-actueel de moeite waard vinden en ons willen ondersteunen om kanker-actueel online te houden dan kunt u ons machtigen voor een periodieke donatie via donaties: https://kanker-actueel.nl/NL/donaties.html of doneer al of niet anoniem op - rekeningnummer NL79 RABO 0372931138 t.n.v. Stichting Gezondheid Actueel in Amersfoort. Onze IBANcode is NL79 RABO 0372 9311 38
Elk bedrag is welkom. En we zijn een ANBI instelling dus uw donatie of gift is in principe aftrekbaar voor de belasting.
En als donateur kunt u ook korting krijgen bij verschillende bedrijven:
29 maart 2016: Bron: Radiat Oncol. 2016; 11: 21. Published online 2016 Feb 11. doi:10.1186/s13014-016-0588-8
In 2014, we analyzed the treatments of the subgroup of patients with tumors that are considered to be in the traditional H&N regions (27 patients and in total 119 treatments of one hour). The target was the CTV of RT and the median CTV size was 63.5 ml. Delivery of power occasionally beyond 1 kW and estimated SAR levels (according to [36]) of on average 72.6 W/kg did not lead to achieving 43 °C. In the 16 patients where interstitial thermometry could be applied, we measured target temperatures up to 38.1–42.3 °C. Hence SAR levels up to four-fold of the SAR delivered in the pelvic region (~16 W/kg) still in cases produced unsatisfactory temperatures, which is a strong indication of the tremendous thermoregulatory response in the H&N region as compared to other regions. Excluding the three patients that were treated in a post-operative setting, a response rate of 53 % was obtained [54]. This response is very promising considering the learning curve and the fact that this was a very unfavorable patient group, i.e. 33 % locally advanced and 67 % re-irradiation. Importantly, no severe complications or enhanced thermal or mucosal toxicities were observed.

in vergelijking met alleen bestraling. En dit is een studie al uit 1988!!!!:
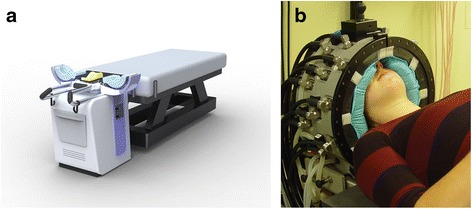
The HYPERcollar redesign improves water bolus shape, stability and skin contact. The renewed positioning strategy allows for positioning of the patient within the required precision of ±5 mm. By clinically introducing the new design, we aim at improving not only treatment quality and reproducibility, but also patient comfort and operator handling, which are all important for a better hyperthermia treatment quality
Status quo and directions in deep head and neck hyperthermia

Abstract
The benefit of hyperthermia as a potent modifier of radiotherapy has been well established and more recently also the combination with chemotherapy was shown beneficial. Also for head and neck cancer, the impact of hyperthermia has been clinically demonstrated by a number of clinical trials. Unfortunately, the technology applied in these studies provided only limited thermal dose control, and the devices used only allowed treatment of target regions close to the skin. Over the last decade, we developed the technology for deep and controlled hyperthermia that allows treatment of the entire head and neck region. Our strategy involves focused microwave heating combined with 3D patient-specific electromagnetic and thermal simulations for conformal, reproducible and adaptive hyperthermia application. Validation of our strategy has been performed by 3D thermal dose assessment based on invasively placed temperature sensors combined with the 3D patient specific simulations. In this paper, we review the phase III clinical evidence for hyperthermia in head and neck tumors, as well as the heating and dosimetry technology applied in these studies. Next, we describe the development, clinical implementation and validation of 3D guided deep hyperthermia with the HYPERcollar, and its second generation, i.e. the HYPERcollar3D. Lastly, we discuss early clinical results and provide an outlook for this technology.
References
Plaats een reactie ...
2 Reacties op "Mond- en keelkanker: Hyperthermie met halsband geeft hoopvolle eerste resultaten bij tumoren in hals en mond bij voorbehandelde kankerpatienten met een recidief"
Gerelateerde artikelen
- Hyperthermie in combinatie met doelgerichte en immuuntherapeutische behandelingen is veel belovende combinatiebehandeling voor kankerpatienten, aldus artsen van ELMEDIX van de universiteit van Antwerpen copy 1
- Matters studie onderzoekt effecten van hyperthermie bij kankerpatienten met solide tumoren en patienten met alvleesklierkanker. copy 1
- Electro hyperthermie naast bestraling verbetert de 5-jaars overleving met 12 procent (79 vs 91 procent) bij patienten met neuskanker. Hyperthermie gaf ook 17 procent meer complete remissies
- Is de Hyperthermie infra rode sauna voor thuisgebruik (META Chamber Infrared Sauna Dome) een goed en veilig alternatief voor total body hyperthermie?
- Hyperthermie plus hoge dosis vitamine C verbetert overall overleving met 40 procent (9 vs 5 maanden) bij zwaar voorbehandelde met vergevorderde niet-kleincellige longkanker in vergelijking met beste zorg
- Hyperthermie heeft vaak therapeutisch effect in combinatie met chemo en bestraling maar blijkt ook effect te hebben op de kankerstamcellen, ook in combinatie met immuuntherapie, blijkt uit reviewstudie
- Hyperthermie plus voedingsprogramma (kytogeen dieet) plus hyperbare zuurstoftherapie aanvullend op chemo geeft uitstekende resultaten op mediane overall overleving (42 maanden) bij patienten met gevorderde niet-kleincellige longkanker
- Hyperthermie studies in overzichtelijk studierapport samengesteld en gepubliceerd door Nederlandse wetenschappers
- Hyperthermie aanvullend op chemo en bestraling geeft gemiddeld 35 procent betere resultaten dan zonder hyperthermie bewijst reviewstudie met meta analyse van 38 gerandomiseerde studies bij verschillende vormen van kanker
- Algemeen: een vergelijking en beschrijving van verschillende hyperthermie systemen zoals die in Nederland en ons omringende landen worden gebruikt.
- Algemeen: Wetenschappelijk artikel over werking en effect van electro-hyperthermie op basis van gepubliceerde studies. Hyperthermie vandaag: Electrische energie een nieuwe kans bij behandeling van kanker
- Meest geavanceerde kliniek ter wereld voor kinderen met kanker - Universiteit van Dusseldorf - neemt nieuwste hyperthermie apparaat in gebruik voor het behandelen van kinderen met kanker met aanvullend hyperthermie.
- Algemeen: Een heet onderwerp: Hyperthermie als een aanvullende behandeling. Wij vertaalden voor u een groot verklarend artikel over hyperthermie als aanvullende behandeling bij gevorderde kanker.
- Algemeen: hyperthermie heeft in een aantal gerandomiseerde studies bewezen significant het effect van chemokuren en bestralingen te vergroten, aldus artikelen uit the Boston Globe en The American Scientist.
- Algemene informatie hyperthermie: Duits academisch ziekenhuis heeft nieuwste hyperthermie apparatuur in gebruik voor specifieke toepassingen bij kanker in de buik, zoals met name voor eierstokkanker, prostaatkanker, baarmoederhalskanker en darmkanker
- Algemeen: Koorts: vriend of vijand? Koorts speelt een cruciale rol in ons immuunssyteem. Onderdrukken van koorts, vooral bij kinderen, lijkt schadelijk voor ons immuunsyteem. het is beter om koorts uit te laten razen.
- Genezing met warmte: Amerikaans wetenschapper verklaart waarom warmte en acute koorts het immuunsysteem stimuleren in het bestrijden van kanker
- Algemeen: Hyperthermie kan effect van chemo en bestraling versterken en beschadigd DNA sneller herstellen, beweren onderzoekers aan de Erasmus en AMC
- Alvleesklierkanker: Hyperthermie bij alvleesklierkanker, een overzicht van huidige stand van zaken en wetenschappelijk bewijs
- Blaaskanker: diepte hyperthermie naast bestraling en chemo na operatie bij blaaskankerpatienten (T1 en T2) met verhoogd risico op recidief geeft goede resultaten op overall overleving en ziektevrije tijd dan zonder zonder hypert
- Baarmoederkanker: Hyperthermie aanvullend naast bestraling bij gevorderde baarmoederhalskankerpatiënten zorgt ook op langere termijn (12 jaar) voor significant betere resultaten.
- Borstkanker: Hyperthermie bij borstkanker: een overzicht van recente studies en artikelen
- Darmkanker: Hyperthermie naast FOLFOX chemo regiem bij gevorderde darmkanker (stadium II tot IV) verdubbelt 5 jaars overleving t.o.v. controlegroep (30 procent t.o. 15 procent
- Eierstokkanker: Totale lichaams hyperthermie naast op platinum gerelateerde chemokuur bij recidief van eierstokkanker geeft hoopgevende resultaten blijkt uit fase II studie.
- Hersentumoren: Hyperthermie met electromagnetische velden bij recidief van hersentumoren (Astrocytoma graad III en Glioblastoma graad IV) geeft significant langere mediane overleving en significant betere kwaliteit van leven,
- Hoofd en hals tumoren: hyperthermie aanvullend naast bestraling geeft significant, 36 procent, meer complete remissies dan alleen bestraling bij tumoren in het hoofd- en halsgebied
- Kiemcel kanker:Hyperthermie in combinatie met chemotherapie zorgt voor een spectaculaire tumorvermindering en een duidelijke verbetering van de overlevingstijd na 5 jaar van kinderen en jongeren met een recidief van kiemcel kanker of resistent tegen chemo
- Longkanker: Hyperthermie naast chemo bij longkanker graad III/ en V geeft hoopvolle resultaten.
- Maagkanker: Combinatiebehandeling van operatie, chemo en inwendige lokale hyperthermie geeft significant meer 2 en 3 jaars overlevingen bij maagkanker
- Melanomen: Hyperthermie van alleen de lymfklieren rondom laatste recidief lijkt effectief maar succes is afhankelijk van stadium van ziekte blijkt uit recente studie. Artikel geplaatst 5 mei 2010
- Mond- en keelkanker: Hyperthermie met halsband geeft hoopvolle eerste resultaten bij tumoren in hals en mond bij voorbehandelde kankerpatienten met een recidief
- Mond- en keelkanker: Hyperthermie naast bestraling van inoperabele lymfklieren ontstaan vanuit mond- en keelkanker (plaveiselcarcinoom) geeft significant minder bijwerkingen en geeft ook significant betere 5-jaars overleving
- Oppervlakkige tumoren: hyperthermie als aanvulling op bestraling geeft significant betere respons bij oppervlakkige tumoren aldus gerandomiseerde studie.
- Prostaatkanker: 75 jarige man met uitgezaaide prostaatkanker in blaaswand en omliggend weefsel pijnvrij en progressievrij door bestraling en hyperthermie copy 1 copy 1
- Prostaatkanker: Nieuw diep hyperthermie systeem gebruikt naast bestraling bij prostaatkankerpatiënten stadium III en IV zorgt voor 3 jaars overleving van 95 procent t.o.v. 60 procent en tot 73 procent vijf jaars overleving.
- Sarcomas en Hyperthermie: Hyperthermie in combinatie met chemotherapie bij soft sarcomas is succesvol blijkt uit fase III studie. Ziektevrije overlevingstijd wordt verdubbeld en mediane overlevingstijd verlengt met ca. 30 procent.
- Hyperthermie, zowel lokaal als totaal blijkt uitstekende en effectieve aanvullende behandeling bij vele vormen van kanker. Hier een aantal artikelen als overzicht.
Dank voor de bespreking van onze nieuwe technologie. Het is goed te weten dat u werkt aan het breder beschikbaar maken en bespreken van de wetenschappelijke kennis.
Inderdaad is al lange tijd bekend dat hyperthermie de effecten van radiotherapie en chemotherapie versterkt, zonder blijvende bijwerkingen meetbaar te versterken. Ook voor het hoofd en hals gebied zijn hiervoor meerdere studies uitgevoerd die de positieve effecten van hyperthermie laten zien.
In het artikel wat u aanhaalt geven wij een overzicht van deze studies, en de gebruikte technologie. De toegepaste apparatuur in de studies is inderdaad veel eenvoudiger dan de apparatuur die wij hebben ontwikkeld (HYPERcollar3D). Maar met een goede reden. Die studies richten zich maar op een deel van het probleem. Met bestaande apparatuur kan maximaal 4 cm van de huid worden verwarmd. Onze technologie kan zowel oppervlakkige tumoren als veel diepere tumoren effectief verwarmen. Zelf dicht bij de hersenen kunnen we de warmte toch nog goed richten. Daarnaast kan de warmte met de HYPERcollar3D worden aangepast aan de patiënt. Met deze aanpak kan zowel de tumor, als omringende uitzaaiingen in de lymfklieren worden behandeld in het hele hoofd-hals gebied. Dit maakt de inzet van hyperthermie potentieel dus veel effectiever. Onze eerste resultaten geven al een eerste indicatie van de winst: voor een groep patiënten met veel slechtere prognose (eerder bestraald) zien we een gelijke tot betere behandeluitkomst.
Hopelijk maakt dit onze aanpak duidelijk. In de komende tijd gaan we werken aan het breder beschikbaar maken van deze technologie. Hiermee hopen we een grote steen bij te dragen aan effectieve en kosteneffectieve gezondheidszorg.
Met vriendelijke groet,
Maarten
PS Overigens heeft Erasmus MC niet gebroken met BSD. Dit is apparatuur die bewezen effectief is en waarmee een bewezen effectieve en kosteneffectieve behandeling kan worden uitgevoerd. Alternatieven voor goede en gecontroleerde hyperthermie behandeling in het bekken gebied zijn nog niet beschikbaar.
Na het operatief wegnemen van mijn amandelen en de basis van de tong heb ik nog enkele uitzaaiingen in mijn nek.
Het vervolgplan zou bestralen en chemo zijn, alleen kijkende naar de permanente schade van het bestralen overweeg ik om toch iets anders te willen proberen.