

Raadpleeg ook:
31 januari 2019: Bron: World J Gastroenterol. 2017 Nov 14; 23(42): 7618–7625.
Opnieuw bewijst een grote studie dat TCM - Traditionele Chinese Medicijnen / Kruiden voor darmkankerpatienten een grote meerwaarde kan betekenen. Hier gaat het om een studie onder 817 darmkankerpatienten met operabele darmkanker stadium I / II / III waarin ook is onderzocht wat het verschil in effect en ziektevrije tijd is tussen rechts en links liggende darmkankertumoren.
Overall blijken TCM - Chinese kruiden mits 6 maanden gebruikt voor een verschil op 6-jaars ziektevrije tijd te geven van 15 procent in vergelijking met geen TCM gebruik. Overall blijkt dat onder de TCM gebruikers met tumoren die links zaten na 6 jaar 56,95 procent nog steeds ziektevrij was tegenover 41,50 procent in de groep die geen TCM - Traditionele Chinese Medicijnen hadden gebruikt.
Voor patienten waar de darmtumoren rechts lagen is dat verschil ook 15 procent in het voordeel van TCM gebruik maar bleken minder patienten ziektevrij op 6 jaar namelijk 52,92 vs 37,19 procent respectievelijk. Statistisch was er dus nauwelijks verschil tussen de tumoren die rechts of links lagen want verschil blijft 15 procent.
En geen van de darmkankerpatienten had chemo of andere behandeling behalve dan operatie gehad.
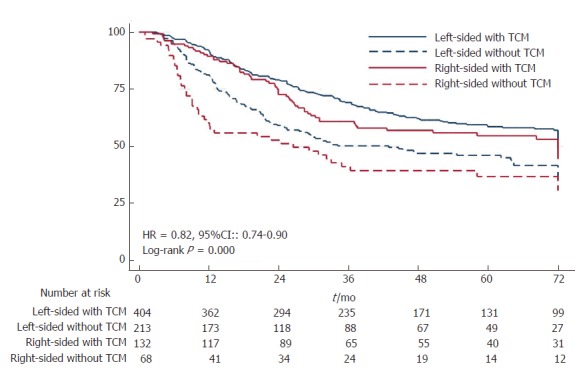
Kaplan-Meier disease-free survival curves for all patients.
Lees eens in oncoline (waar de officiele behandelingsrichtlijnen worden gegeven voor alle vormen van kanker) wat de prognose is voor operabele darmkanker dan schrikt u denk ik van de prognoses, zelfs met chemo.
Bedenk dat er een therapeutisch effect van 15 procent is op wel of geen recidief tussen wel of geen TCM gebruik. Welke reguliere behandeling bereikt dat?
Hier het abstract van deze studie: Right- and left-sided colorectal cancers respond differently to traditional Chinese medicine met verwijzingen naar referenties die volledig gratis is in te zien en met gedetailleerde grafieken.
Patients with either LSCRC or RSCC and who took TCM experienced longer DFS; furthermore, patients with RSCC benefited more from TCM in DFS.
Right- and left-sided colorectal cancers respond differently to traditional Chinese medicine
Abstract
AIM
To explore the differences in the responses of left-sided colorectal cancer (LSCRC) and right-sided colon cancer (RSCC) to traditional Chinese medicine (TCM).
METHODS
Patients with postoperative stage I-III colorectal cancer (CRC) were enrolled and divided into the LSCRC with or without TCM and RSCC with or without TCM groups depending on the primary tumor side and TCM administration. Patients in the TCM group were given TCM for at least 6 mo. Our research adopted disease-free survival (DFS) as the primary endpoint. We applied a Cox proportional hazards regression model for the multivariate factor analysis using Stata 12.0 and SPSS 22.0 software for data analysis.
RESULTS
Of the 817 patients included in our study, 617 had LSCRC (TCM group, n = 404; Non-TCM group, n = 213), and 200 had RSCC (TCM group, n = 132; Non-TCM group, n = 68). The 6-year DFS for patients with LSCRC was 56.95% in the TCM group and 41.50% in the Non-TCM group (P = 0.000). For patients with RSCC, the 6-year DFS was 52.92% in the TCM group and 37.19% in the Non-TCM group (P = 0.003). Differences between LSCRC and RSCC were not statistically significant regardless of TCM ingestion.
CONCLUSION
Patients with either LSCRC or RSCC and who took TCM experienced longer DFS; furthermore, patients with RSCC benefited more from TCM in DFS.
Research perspectives
Recent studies have proposed that location of primary tumor was related to recurrence, metastasis and the therapeutic effect. The author’s results indicated that patients with LSCRC and RSCC responded differently to TCM; those with RSCC benefited more from TCM than those with LSCRC. Thus, TCM was recommended to postoperative patients with CRC of both sides, especially the right side. In the future research, CRC should be treated separately based on the primary tumor sides.
Footnotes
Manuscript source: Unsolicited manuscript
Specialty type: Gastroenterology and hepatology
Country of origin: China
Peer-review report classification
Grade A (Excellent): A
Grade B (Very good): B
Grade C (Good): 0
Grade D (Fair): D
Grade E (Poor): 0
Institutional review board statement: The study was reviewed and approved by IRB of Shuguang Hospital affiliated with Shanghai University of TCM.
Informed consent statement: All study participants, or their legal guardian, provided informed written consent prior to study enrollment.
Conflict-of-interest statement: All authors have declared no conflicts of interest.
Data sharing statement: No additional data were available.
Peer-review started: July 5, 2017
First decision: August 30, 2017
Article in press: September 26, 2017
P- Reviewer: Jeong KY, Mavridis K, Liao KF S- Editor: Chen K L- Editor: A E- Editor: Ma YJ
Contributor Information
Shan-Shan Liu, Oncology Department of Shanghai Municipal Hospital of Traditional Chinese Medicine, Shanghai University of Traditional Chinese Medicine, Shanghai 200071, China.
Qi Shi, Oncology Department of Shanghai Municipal Hospital of Traditional Chinese Medicine, Shanghai University of Traditional Chinese Medicine, Shanghai 200071, China.
Hong-Jia Li, Oncology Department of Shanghai Municipal Hospital of Traditional Chinese Medicine, Shanghai University of Traditional Chinese Medicine, Shanghai 200071, China.
Wei Yang, Oncology Department of Shanghai Municipal Hospital of Traditional Chinese Medicine, Shanghai University of Traditional Chinese Medicine, Shanghai 200071, China.
Su-Su Han, Oncology Department of Shanghai Municipal Hospital of Traditional Chinese Medicine, Shanghai University of Traditional Chinese Medicine, Shanghai 200071, China.
Shao-Qi Zong, Oncology Department of Shanghai Municipal Hospital of Traditional Chinese Medicine, Shanghai University of Traditional Chinese Medicine, Shanghai 200071, China.
Wen Li, Oncology Department of Shanghai Municipal Hospital of Traditional Chinese Medicine, Shanghai University of Traditional Chinese Medicine, Shanghai 200071, China.
Feng-Gang Hou, Oncology Department of Shanghai Municipal Hospital of Traditional Chinese Medicine, Shanghai University of Traditional Chinese Medicine, Shanghai 200071, China. nc.hs.yzs@7211.
References
Articles from World Journal of Gastroenterology are provided here courtesy of Baishideng Publishing Group Inc
Gerelateerde artikelen
- Chinese kruidencombinatie PRM1201 geeft in combinatie met chemotherapie na 3 jaar 9 procent betere ziektevrije overleving bij patienten met operabele darmkanker stadium III
- TCM - Traditionele Chinese Medicijnen / Kruiden verbeteren ziektevrije tijd met 15 procent voor operabele darmkanker stadium III in vergelijking met geen TCM. Darmtumoren aan linkerkant hadden beste ziektevrije tijd 56 vs 42 procent voor geen TCM
- ShenQi FuZheng Injectie aanvullend op chemotherapie bij darmkankerpatienten verbetert overall overleving, verbetert immuunwaarden en vermindert de bijwerkingen bewijst een meta-analyse
- TCM - Traditionele Chinese Medicijnen (Chinese kruiden) al of niet naast chemo bij operabele darmkanker stadium II en III geven veel betere ziektevrije tijd en overall overleving op 5 jaar dan zonder TCM. copy 1
- Chinese Kruiden - TCM alleen of aanvullend op westerse aanpak van darmkanker stadium II en III verminderen kans op recidief met 39 procent op 5-jaars meting in vergelijking met alleen westerse aanpak van chemo en bestraling
- Chinese kruiden - Shenqui - als aanvulling bij RFA behandeling van levertumoren geeft significant betere resultaten in alle opzichten: betere kwaliteit van leven, sneller herstel na RFA behandeling en een significant betere en langere overleving
- Goshajinkigan - Japans kruidenmengsel - vermindert significant de perifere neurotoxiteit veroorzaakt door oxaliplatin bij uitgezaaide darmkanker
- Chinese kruiden: Injecties met Shenmai als aanvulling op chemokuren cisplatin en 5-FU bij gevorderde darmkanker geeft een significant betere 5 jaars ziektevrije tijd en significant betere kwaliteit van leven
Plaats een reactie ...
2 Reacties op "TCM - Traditionele Chinese Medicijnen / Kruiden verbeteren ziektevrije tijd met 15 procent voor operabele darmkanker stadium III in vergelijking met geen TCM. Darmtumoren aan linkerkant hadden beste ziektevrije tijd 56 vs 42 procent voor geen TCM"