

Mocht u kanker-actueel de moeite waard vinden en ons willen ondersteunen om kanker-actueel online te houden dan kunt u ons machtigen voor een periodieke donatie via donaties: https://kanker-actueel.nl/NL/donaties.html of doneer al of niet anoniem op - rekeningnummer NL79 RABO 0372931138 t.n.v. Stichting Gezondheid Actueel in Amersfoort. Onze IBANcode is NL79 RABO 0372 9311 38
Elk bedrag is welkom. En we zijn een ANBI instelling dus uw donatie of gift is in principe aftrekbaar voor de belasting. En als donateur kunt u ook korting krijgen bij verschillende bedrijven:
16 januari 2017:
De NAS - National Academies Press heeft een boek: The Health Effects of Cannabis and Cannabinoids:
The Current State of Evidence and Recommendations for Research
uitgebracht over de huidige status van cannabis en cannabis olie en cannabinoiden, stofjes uit marihuana. Het boek kunt u downloaden via deze PDF: Cannabis boek met wetenschappeljk bewijs
Het hoofdstuk over cannabis bij kanker kunt u als PDF downloaden: Cannabis bij kanker
13 januari 2017:
Zelf heb ik geen enkele ervaring met cannabis of wietolie enz. Alle informatie hierover in gerelateerde artikelen is via studies of internet verzameld. Nu proberen steeds mensen gratis reclame te maken waar de cannabis en wietolie, THC of CBD enz. te koop is.
Hier de websites waar zover ik weet cannabis - marihuana, wietolie , TCH en CBD te koop is. Wij hebben bij geen enkel adres een belang of contacten. Dus welke de beste is durf ik niet te zeggen. Maar dat kunt u verder zelf wel beoordelen hoop ik. lees verder ook onze disclaimer.
Websites in willekeurige volgorde:
Maripharm.nl
Mediwiet waarschijnlijk de bekendste maar ook met de agressiefste marketingmethodes zoals reacties via klanten op internet en min of meer verbonden aan Rick Simpson en m.i. onbewezen claims als zou cannabis ook kanker kunnen genezen.
THC olie .nl waar mensen biologische THC kunnen bestellen bij individuele telers, zeggen ze. Of dit een slimme constructie is om zelf rijk van te worden durf ik niet te zeggen.
En de Transvaal apotheek waar u medische cannabis en / of cannabisolie kunt bestellen.
3 september 2015: Bron: Br J Clin Pharmacol. 2013 Feb;75(2):303-12. doi: 10.1111/j.1365-2125.2012.04298.x
Cannabidiol als potentieel anti-kanker medicijn
Ik heb een link naar dit studierapport al in verschillende artikelen over cannabis verwerkt. Maar het lijkt me goed dit ook nog eens apart te vermelden. Dit rapport geeft een mooi overzicht van de werking van CPD en THC bij kanker en de stand van zaken in het onderzoek daarnaar. Ik heb de conclusie uit dit rapport zo goed als mogelijk letterlijk vertaald in het Nederlands met hulp van google translation.
Conclusie/discussie:
Samenvattend; de niet-psychoactieve (= je wordt er niet stoned van geloof ik dat hiermee wordt bedoeld) plantaardige cannabinoïde CBD vertoont pro-apoptotische (= stimuleert apoptose / zelfdoding van kankercellen) en antiproliferatieve (= verhindert aanzet tot vorming van DNA mutaties) activiteiten in verschillende typen tumoren en kunnen ook anti-migratie, anti-invasieve, anti-metastatische (= geen uitzaaiingen) eigenschappen bevorderen en misschien ook anti-angiogene (tegengaan van vorming van bloedvaten) eigenschappen. Op basis van deze resultaten, lijkt dit bewijsmateriaal te suggereren dat CBD een krachtige remmer kan zijn van zowel de groei en de verspreiding/uitzaaiingen van kanker.
Interessant is dat de antikanker werking van deze verbinding selectief lijkt te zijn voor kankercellen, tenminste in vitro (=in laboratoriumsetting), aangezien het geen invloed uitoefent op de normale cellijnen. De werkzaamheid van CBD is gekoppeld aan de mogelijkheid om meerdere cellulaire routes (= mutaties) te beïnvloeden, waarmee tumorgenese (=tumorvorming) gepaard gaat, door de modulering van verschillende intracellulaire pathways/paden. Dit is wel afhankelijk van het soort kanker. Het meest voorkomende effect van CBD is de toename van de ROS productie die bepalend lijkt voor het veroorzaken van de gunstige effecten bij de onderzochte typen van kankercellen. De rol van de cannabinoïde / vanilloid op de receptoren door de CBD effecten is meer omstreden. In sommige gevallen (longkanker, leukemie, darmkanker) is er een duidelijke bijdrage van deze receptoren aangetoond door het gebruik van specifieke antagonisten, maar in andere kankersoorten (gliomen en borsttumoren) lijkt de relevantie alleen marginaal of afwezig zijn. Naast de in vitro data, werd de werkzaamheid van CBD in het verminderen van tumorgroei en, in sommige gevallen, voorkomen / verminderen van uitzaaiingen / metastasering bevestigd in experimentele dierstudies..jpg)
Foto: CBD effect bij borstkanker
Echter, de mogelijke klinische toepassing van CBD in een kankerbehandeling verdient meer aandacht. De lage toxiciteit is zeker een goed uitgangspunt. CBD gedraagt zich als een niet giftige stof; want orale toediening van CBD 700 mg per dag gedurende 6 weken veroorzaakt geen enkele openlijke toxiciteit / bijwerkingen bij de mens en suggereert dat een mogelijke langdurige behandeling tot de mogelijkheden behoort. De manier van toediening lijkt problematischer omdat orale absorptie van CBD traag en onvoorspelbaar verloopt. Echter, een 6 weken orale CBD behandeling 10 mg kg-per dag veroorzaakte een gemiddelde plasmaconcentratie van CBD tussen de 6 en 11 ng ml-1 (ongeveer 0,036 um) die niet veel verschilde van de hoeveelheid die 6 weken lang werd toegediend. Interessant is dat met deze concentratie werd aangetoond dat er actief invasieve longkanker mee werd voorkomen [52, 53], wat erop wijst dat in sommige gevallen de orale route de geschikte keuze van toediening kan zijn.
Bovendien bleek uit experimentele gegevens dat de gecombineerde behandeling met CBD en Δ9-THC effectiever is in het verminderen van de proliferatie van kankercellen, wat suggereert dat de gelijktijdige toediening een betere keuze voor kankertherapie zou kunnen zijn. Bovendien is een oromucosale behandeling (= via een spray of zuigtablet) met Sativex ™ 10 mg (een preparaat met een 1: 1 verhouding tussen CBD en Δ9-THC, en onlangs goedgekeurd voor multiple sclerose) in een plasmaconcentratie van CBD effectief in het verminderen van long invasie in vitro. De aldus met Sativex ™ bereikte resultaten suggereren dat het gebruik van verschillende mengingen van fytocannabinoïden (= plantaardige cannabinoiden) in een variabele verhouding zou kunnen leiden tot een beter resultaat zonder farmacokinetische (= chemische stoffen) interactie . Bovendien kan oromucosale toediening ook eerste keuze zijn wanneer eer sprake is van misselijkheid en braken.
.jpg)
Tot slot kan het gebruik van CBD / Sativex in combinatie met klassieke chemokuren worden voorgesteld om te controleren of er sprake is van een synergistisch effect (= elkaar versterkend effect) , waardoor er wellicht gekozen kan worden voor een verlaging van deklinische chemo dosering, waardoor er minder bijwerkingen optreden met behoud van de effectiviteit. In het licht van de veiligheid en gezien het feit dat CBD momenteel al wordt gebruikt bij patiënten met multiple sclerose, suggereren de bevindingen hier samengevat dat CBD serieuze aandacht verdient voor toepassing in een behandeling van kanker.
Het volledige studierapport: Cannabidiol as potential anticancer drug waaruit ik de conclusie heb vertaald is gratis in te zien met uitstekende referentielijst.
13 januari 2017:
Zelf heb ik geen enkele ervaring met cannabis of wietolie enz. Alle inforamtie hierover in gerelateerde artikelen is via studies of internet verzameld. Nu proberen steeds mensen gratis reclame te maken waar de cannabis en wietolie, THC of CBD enz. te koop is.
Hier de websites waar zover ik weet cannabis - marihuana, wietolie , TCH en CBD te koop is. Wij hebben bij geen enkel adres een belang of contacten. Dus welke de beste is durf ik niet te zeggen. Maar dat kunt u verder zelf wel beoordelen hoop ik. lees verder ook onze disclaimer.
Websites in willekeurige volgorde:
Maripharm.nl
Mediwiet waarschijnlijk de bekendste maar ook met de agressiefste marketingmethodes zoals reacties via klanten op internet en min of meer verbonden aan Rick Simpson en m.i. onbewezen claims als zou cannabis ook kanker kunnen genezen.
THC olie .nl waar mensen biologische THC kunnen bestellen bij individuele telers, zeggen ze. Of dit een slimme constructie is om zelf rijk van te worden durf ik niet te zeggen.
Hier het abstract van de studie plus conclusie plus referentielijst:
In the light of its safety record and considering that CBD is already currently used in patients with multiple sclerosis, the findings here summarized suggest that CBD might be worthy of clinical consideration for cancer therapy.
Cannabidiol as potential anticancer drug
Abstract
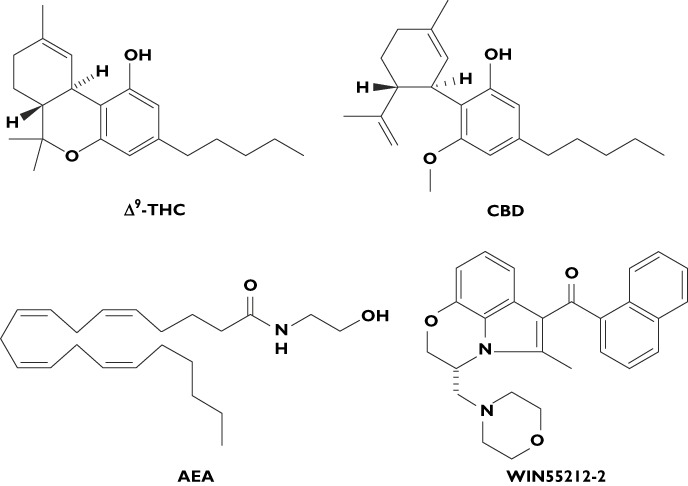
Over the past years, several lines of evidence support an antitumourigenic effect of cannabinoids including Δ9-tetrahydrocannabinol (Δ9-THC), synthetic agonists, endocannabinoids and endocannabinoid transport or degradation inhibitors. Indeed, cannabinoids possess anti-proliferative and pro-apoptotic effects and they are known to interfere with tumour neovascularization, cancer cell migration, adhesion, invasion and metastasization. However, the clinical use of Δ9-THC and additional cannabinoid agonists is often limited by their unwanted psychoactive side effects, and for this reason interest in non-psychoactive cannabinoid compounds with structural affinity for Δ9-THC, such as cannabidiol (CBD), has substantially increased in recent years. The present review will focus on the efficacy of CBD in the modulation of different steps of tumourigenesis in several types of cancer and highlights the importance of exploring CBD/CBD analogues as alternative therapeutic agents.
Conclusion and future directions
Collectively, the non-psychoactive plant-derived cannabinoid CBD exhibits pro-apoptotic and anti-proliferative actions in different types of tumours and may also exert anti-migratory, anti-invasive, anti-metastatic and perhaps anti-angiogenic properties. On the basis of these results, evidence is emerging to suggest that CBD is a potent inhibitor of both cancer growth and spread.
Interestingly, the anticancer effect of this compound seems to be selective for cancer cells, at least in vitro, since it does not affect normal cell lines. The efficacy of CBD is linked to its ability to target multiple cellular pathways that control tumourigenesis through the modulation of different intracellular signalling depending on the cancer type considered. The most common effect of CBD is the increase in ROS production that seems to be determinant for triggering its beneficial action in all the considered cancer cell types. The role of cannabinoid/vanilloid receptors in mediating CBD effects is more controversial. In some cases (lung, leukaemia, colon) a clear contribution of these receptors has been demonstrated through the use of specific antagonists, but in other cancer types (glioma and breast) their relevance appears only marginal or absent. Besides the in vitro data, the efficacy of CBD in reducing tumour growth and, in some cases, metastasization was confirmed in experimental animal models. However, the potential clinical application of CBD for cancer therapy needs some consideration. Its low toxicity is certainly a good starting point. CBD behaves as a non toxic compound; indeed oral administration of CBD 700 mg day−1 for 6 weeks did not show any overt toxicity in humans [59] suggesting its possible exploitation for prolonged treatment. The route of administration appears more problematic since CBD oral absorption is slow and unpredictable. However, 6 weeks of oral CBD treatment 10 mg kg−1 day−1 provoked a mean plasma concentration of CBD between 6 and 11ng ml−1 (about 0.036 µm) [60] that did not differ significantly over the 6 weeks of administration. Interestingly, this range of concentration was demonstrated to be active in inhibiting lung cancer cell invasion [52, 53], thus suggesting that in some cases the oral route could be the appropriate choice. Additionally, experimental data showed that combined treatment with CBD and Δ9-THC could be more effective in reducing cancer cell proliferation, suggesting that the co-administration may represent a better choice for cancer therapy. Accordingly, oromucosal treatment with Sativex™ 10 mg (a formulation with a 1:1 ratio of CBD and Δ9-THC, recently approved for multiple sclerosis) resulted in a CBD plasma concentration of effective in reducing lung cell invasion in vitro. Thus, the results obtained with Sativex™ suggest that the use of different associations of phytocannabinoids in a variable proportion might lead to a better outcome without pharmacokinetic interaction [61]. Moreover, oromucosal administration may represent a first choice in the presence of nausea and vomiting. Finally, the use of CBD/Sativex can be suggested in combination with classical chemotherapeutic agents to check for the presence of a synergistic effect that might potentially allow clinical chemotherapeutic dose reduction, thereby reducing toxicity while maintaining efficacy. In the light of its safety record and considering that CBD is already currently used in patients with multiple sclerosis, the findings here summarized suggest that CBD might be worthy of clinical consideration for cancer therapy.
references:
Plaats een reactie ...
1 Reactie op "Cannabisstofjes CBD en THC verdienen meer aandacht als toepassing in een behandeling van kanker blijkt uit review studie"
Gerelateerde artikelen
- Cannabis - marihuana gebruik vergroot risico op Alzheimer - dementie blijkt uit 14 jarige studie onder meer dan 6 miljoen mensen
- Legalisatie van medische marihuana gunstig voor kankerpatiënten. Minder morfine nodig en minder aan pijn gerelateerde ziekenhuisopnames
- Medicinale cannabis verlicht langdurig pijn bij patienten met chronische pijn, blijkt uit kleine Harvard studie.
- UMCG Groningen gaat onderzoek doen naar effecten van wietolie - cannabis na twee genezen leverkankerpatienten
- Nieuwe overzichtsstudie van de rol die cannabis, marihuana kan spelen in de zorg voor kankerpatienten geeft uitstekend overzicht van stand van zaken
- Medicinale wiet (cannabis - marihuana) vermindert pijnklachten en laat Amerikaanse werknemers ouder dan 50 jaar langer werken na legalisering van de cannabis, blijkt uit 10-jarig onderzoek
- Cannabis gebruik met hoge THC gehaltes leidt tot meer psychoses op latere leeftijd aldus nieuw wetenschappelijk onderzoek
- Recreatief gebruik van marihuana - cannabis sativa verbetert kwaliteit van leven ( depressie, pijn, angst, eetlust) bij nieuw gediagnosteerden van mond- en keelkanker
- 80 procent van amerikaanse oncologen bespreken medische marihuana met hun patienten maar de meesten doen dat zonder voldoende kennis over de effecten en bijwerkingen van medische cannabis
- DE WATERKOKER VAN MIJN TANTE Een verhaal over medicinale cannabis
- Waar kan ik marihuana of cannabis kopen?
- Cannabisstofjes CBD en THC verdienen meer aandacht als toepassing in een behandeling van kanker blijkt uit review studie
- Cannabis olie - wietolie moet wel zorgvuldig geproduceerd en verwarmd worden anders kan het juist schadelijk zijn en kankergroei stimuleren, blijkt uit Nederlandse studie
- Cannabis - marihuana toegevoegd aan opiaten zoals morfine en oxycodon verhoogt pijnstillende effect bij patiënten met chronische pijn en zij hebben daardoor minder morfine c.q. oxycodon nodig
- Cannabis - THC CBD extract geeft 30 procent meer verlichting van pijn bij patiënten met vergevorderde kanker als de pijn niet meer alleen met opiaten als morfine is op te lossen.
- Marihuana - Cannabis verzacht zenuwpijnen (neuropathische pijn) en verbetert slaap en vermindert angstige en depressieve gevoelens blijkt uit een gerandomiseerde kleinschalige studie
- Cannabis - marihuana stimuleert eetlust en verbetert smaak voor kankerpatienten.
- Marihuana - cannabis als medicijn en als pijnstiller en wellicht als medicijn bij Alzheimer - dementie
CBD olie blijkt steeds meer toepassingsgebieden te hebben, zie hier:
https://www.medicinalewietolie.com/waar-is-cbd-olie-goed-voor.html
Overleg ALTIJD met een arts.
Met vriendelijke groet,
MedicinaleWietOlie.com
https:/www.medicinalewietolie.com/