

Mocht u kanker-actueel de moeite waard vinden en ons willen ondersteunen om kanker-actueel online te houden dan kunt u ons machtigen voor een periodieke donatie via donaties: https://kanker-actueel.nl/NL/donaties.html of doneer al of niet anoniem op - rekeningnummer NL79 RABO 0372931138 t.n.v. Stichting Gezondheid Actueel in Amersfoort. Onze IBANcode is NL79 RABO 0372 9311 38
Elk bedrag is welkom. En we zijn een ANBI instelling dus uw donatie of gift is in principe aftrekbaar voor de belasting.
En als donateur kunt u ook korting krijgen bij verschillende bedrijven:
26 april 2016: Bron: ASCO 2016
Wanneer bij een recidief van eierstokkanker operatief debulking wordt toegepast waarbij de resttumoren niet groter blijven dan 1 cm. dan stijgt mediaan overall overleving met vele maanden / enkele jaren als tijdens de debulking een hipec wordt toegepast in vergelijking met resttumoren die groter dan 1 cm. blijven / zijn. Dit geldt ook voor primaire buikvlieskanker.
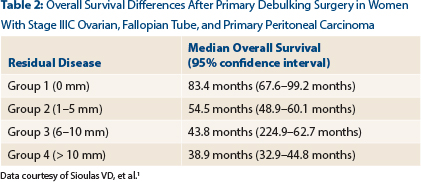
Debulking plus hipec geeft mediaan 65.1 maanden versus 40.6 maanden overall overleving. Voor de hele groep patiënten waarvan ca. 42% een debulking plus hipec kreeg en de anderen chemo achteraf bleek de mediane overall overleving 54.7 maanden (95% CI = 50.8–58.7 months). De chemo die werd gebruikt is of een hipec of de meest gebruikte chemo bij eierstokkanker taxol plus carboplatin. Zie hier de verschillen uit de vier groepen uit de fase III studie.
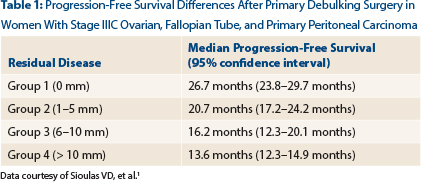
Ook ziektevrije tijd was beter voor debulking tot 1 cm. of minder:
Het is dus alleszins de moeite waard om bij een recidief van eierstokkanker te kijken of er toch een debulking kan worden toegepast, zelfs als bij resistentie na aanvankelijk een goed aanslaan van de chemo de tumormarkers weer oplopen en er kleine tumoren ontstaan.
Bovenstaande resultaten zijn gerelateerd aan drie studies, waarvan de fase III studie op ASCO 2016 als nieuw werd gepresenteerd, klik op de links en u kunt de abstracten lezen. alleen in de eerste link krijgt u alle abstracten van ASCO 2016 en is wel heel veel. Abstract 26 gaat over genoemde atudie.
Bovenstaande heb ik uit dit artikel uit de ASCOpost gehaald:
References
Mutaties bepalen wel of niet aanslaan van behandeling:
Interessanter wordt het nog als er vooraf een receptoren en mutatieonderzoek wordt gedaan, want wie een bepaalde mutatie heeft en daaronder vallen ook BRCA 1 en BRCA 2, hebben meer kans op het aanslaan van bv. chemo plus avastin dan patiënten zonder aanwijsbare mutaties. Zie deze studie die op ASCO 2016 ook werd gepresenteerd:
In a study exploring the effect of primary debulking surgery in women with bulky stage IIIC ovarian, fallopian tube, and primary peritoneal cancers, cytoreduction to no gross residual disease was associated with the best survival outcomes.1 Cytoreduction to 1 to 10 mm of residual disease was also associated with survival benefit as compared to residual disease greater than 10 mm.
PDS versus neoadjuvant chemotherapy
Gerelateerde artikelen
- Lymfklieren weghalen bij operatieve verwijdering van eierstokkanker geeft geen betere overall overleving maar wel meer ernstige complicaties en meer doden gerelateerd aan de operatie
- Debulkingoperatie tot 1 cm of minder plus chemotherapie of hipec geeft veel betere ziektevrije tijd en overall overleving bij recidief van eierstokkanker en primaire buikvlieskanker
- Nieuwe chirurgische aanpak via kijkoperatie welke de volgorde van chemo en / of operatie bepaalt verbetert spectaculair - 68% beter - de overall overleving van patiënten met eierstokkanker.
- Operatie: Cryosurgery (bevriezen of verhitten) van uitzaaiingen - ook in andere organen - blijkt voor uitstekende resultaten te zorgen op de overlevingsduur en kwaliteit van leven bij patienten met eierstokkanker stadium 3 en 4
- Lymfklieren weghalen bij operatieve verwijdering van eierstokkanker geeft geen betere overall overleving maar wel meer ernstige complicaties en meer doden gerelateerd aan de operatie copy 1
- Operatie bij recidief van eierstokkanker (2e operatieve ingreep dus) significant levensverlengend en succesvol uitgevoerd bij ca. 200 patiënten met recidief van eierstokkanker verdeeld over drie gerandomiseerde studies
Plaats een reactie ...
Reageer op "Debulkingoperatie tot 1 cm of minder plus chemotherapie of hipec geeft veel betere ziektevrije tijd en overall overleving bij recidief van eierstokkanker en primaire buikvlieskanker"