Kanker Actueel maakt gebruik van cookies om ons websiteverkeer te analyseren om u een optimale bezoekerservaring te bieden. Bovendien plaatsen adverteerders tracking cookies om u gepersonaliseerde advertenties te tonen. Door op [OK] te klikken gaat u hiermee akkoord.
Alvleesklierkanker en galwegenkanker zijn een van de moeilijkst te behandelen vormen van kanker. Maar ook bij deze vormen van kanker blijkt een personalised aanpak op basis van DNA en RNA mutaties meer en meer de beste aanpak te kunnen zijn. (zie ook gerelateerde artikelen). Een onderzoeksteam van Nature Research maakte een overzichtsstudie over de ontwikkelingen binnen personalised medicine specifiek voor galwegenkanker en publiceerde dat eind vorig jaar in Precision Medicin.
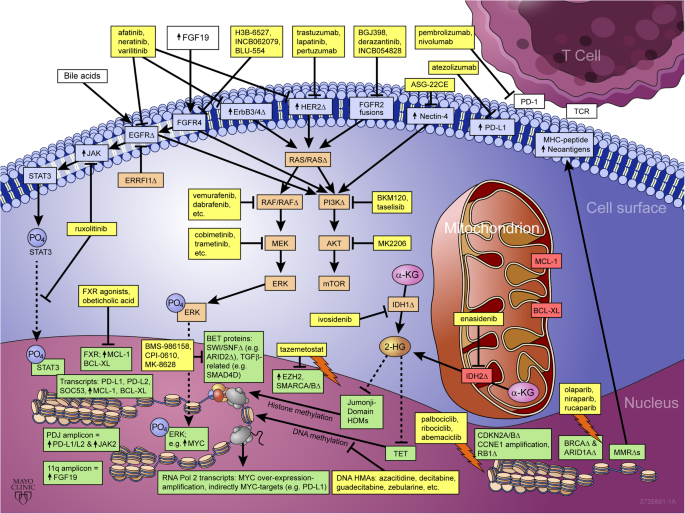
Het studie rapport: Emerging role of precision medicine in biliary tract cancers is gratis in te zien en de onderzoekers bespreken een aantal veel voorkomende DNA en RNA mutaties en de daarop gerichte behandelingen waaronder immuuntherapie met anti-PD medicijnen. Hier een grafiek uit die studie van hoeveel mutaties er wel niet zijn.
Fig. 1
Emerging role of precision medicine in biliary tract cancers. Yellow boxes highlight US FDA-approved drugs and drugs undergoing clinical investigation as reviewed, with arrows indicating pathway/target activation and blocked lines indicating pathway/target inhibition. BTC targets/pathways discussed are shown in color-coded boxes according to subcellular localization, blue = cell surface, orange = cytsolic, red = mitochondrial, and green = nuclear. “↑” denotes over-expression, “Δ” denotes copy number abbreation and/or point mutation, a lighting bolt symbol denotes a synthetic lethal interaction between drug(s) and target(s) listed
Ik zal het studierapport niet verder vertalen. Hier het abstract van de studie met de referentielijst en lees anders verder het volledige artikel in Precision Medicin.
Biliary tracts cancers (BTCs) are a diverse group of aggressive malignancies with an overall poor prognosis. Genomic characterization has uncovered many putative clinically actionable aberrations that can also facilitate the prognostication of patients. As such, comprehensive genomic profiling is playing a growing role in the clinical management of BTCs. Currently however, there is only one precision medicine approved by the US Food and Drug Administration (FDA) for the treatment of BTCs. Herein, we highlight the prevalence and prognostic, diagnostic, and predictive significance of recurrent mutations and other genomic aberrations with current clinical implications or emerging relevance to clinical practice. Some ongoing clinical trials, as well as future areas of exploration for precision oncology in BTCs are highlighted.
Conclusions
While treatment of MSI-H/dMMR tumors with pembrolizumab is currently the only targeted, biomarker-based therapy FDA-approved for BTCs, there are many potentially actionable aberrations in BTCs, and comprehensive genomic profiling is highly recommended in the management of BTCs. Additional biomarker-based treatments such as NTRK/ROS1-targeted therapies, albeit very low prevalence in BTCs, and FGFR-targeted therapies, are likely candidates for near-term regulatory approvals. There are several targeted therapies FDA-approved for other indications (e.g., HER2-targeted agents) with potential relevance for precision oncology application in BTCs that could possibly be considered for off-label use on a case-by-case basis. Importantly, there are also several biomarker-driven and unselected clinical trials for many of these FDA-approved agents to expand into BTCs, as well as for novel targeted therapies, that should be watched and considered for enrollment. Biomarker-driven umbrella or basket trials will be of high interest to BTC research efforts, as well as facilitating the development of novel targeted agents and combinations thereof. Many of the mutations/aberrations observed in BTCs are often indolent drivers alone (e.g., IDH or FGFR2), and even where such drivers may be significantly beneficial to target as monotherapy, combination therapy targeting two or more drivers is likely to yield deeper and more durable responses. Well-designed preclinical models, that recapitulate in vivo properties and thus can accurately interrogate precise genomic contexts to derive and test such combination therapies, will be paramount in moving beyond empirical therapy into a new era of precision therapy for BTCs.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References belonging to emerging role of precision medicine in biliary tract cancers
References
1.
Razumilava, N. & Gores, G. J. Building a staircase to precision medicine for biliary tract cancer. Nat. Genet.47, 967 (2015).
Hendriks, Y. M. et al. Diagnostic approach and management of Lynch syndrome (hereditary nonpolyposis colorectal carcinoma): a guide for clinicians. Cancer J. Clin.56, 213–225 (2006).
Cortes-Ciriano, I., Lee, S., Park, W. Y., Kim, T. M. & Park, P. J. A molecular portrait of microsatellite instability across multiple cancers. Nat. Commun.8, 15180 (2017).
Herman, J. G. et al. Incidence and functional consequences of hMLH1 promoter hypermethylation in colorectal carcinoma. Proc. Natl Acad. Sci. USA95, 6870–6875 (1998).
Ligtenberg, M. J. et al. Heritable somatic methylation and inactivation of MSH2 in families with Lynch syndrome due to deletion of the 3′ exons of TACSTD1. Nat. Genet.41, 112–117 (2009).
Chalmers, Z. R. et al. Analysis of tumor mutation burden (TMB) in >51,000 clinical cancer patients to identify novel non-coding PMS2 promoter mutations associated with increased TMB. J. Clin. Oncol.34, 9572–9572 (2016).
Lemery, S., Keegan, P. & Pazdur, R. First FDA approval agnostic of cancer site—when a biomarker defines the indication. N. Engl. J. Med377, 1409–1412 (2017).
Umar, A. et al. Revised Bethesda Guidelines for hereditary nonpolyposis colorectal cancer (Lynch syndrome) and microsatellite instability. J. Natl Cancer Inst.96, 261–268 (2004).
Goodman, A. M. et al. Tumor mutational burden as an independent predictor of response to immunotherapy in diverse cancers. Mol. Cancer Ther.16, 2598–2608 (2017).
Sabbatino, F. et al. PD-L1 and HLA Class I antigen expression and clinical course of the disease in intrahepatic cholangiocarcinoma. Clin. Cancer Res.22, 470–478 (2016).
Bang, Y. J. et al. 525 Safety and efficacy of pembrolizumab (MK-3475) in patients (pts) with advanced biliary tract cancer: interim results of KEYNOTE-028. Eur. J. Cancer51, S112.
19.
Barrett, M. T. et al. Genomic amplification of 9p24.1 targeting JAK2, PD-L1, and PD-L2 is enriched in high-risk triple negative breast cancer. Oncotarget6, 26483–26493 (2015).
Green, M. R. et al. Integrative analysis reveals selective 9p24.1 amplification, increased PD-1 ligand expression, and further induction via JAK2 in nodular sclerosing Hodgkin lymphoma and primary mediastinal large B-cell lymphoma. Blood116, 3268–3277 (2010).
Guagnano, V. et al. Discovery of 3-(2,6-dichloro-3,5-dimethoxy-phenyl)-1-{6-[4-(4-ethyl-piperazin-1-yl)-phenylamin o]-pyrimidin-4-yl}-1-methyl-urea (NVP-BGJ398), a potent and selective inhibitor of the fibroblast growth factor receptor family of receptor tyrosine kinase. J. Med. Chem.54, 7066–7083 (2011).
Javle, M. et al. Phase II Study of BGJ398 in patients with FGFR-altered advanced cholangiocarcinoma. (2017). J Clin Oncol. 10.1200/JCO.2017.75.5009.
29.
Gilbert, J. A. BGJ398 for FGFR-altered advanced cholangiocarcinoma. Lancet Oncol. 10.1016/S1470-2045(17)30902-6 (2017).
30.
Perwad, F., Zhang, M. Y., Tenenhouse, H. S. & Portale, A. A. Fibroblast growth factor 23 impairs phosphorus and vitamin D metabolism in vivo and suppresses 25-hydroxyvitamin D-1alpha-hydroxylase expression in vitro. Am. J. Physiol. Ren. Physiol.293, F1577–F1583 (2007).
Gattineni, J. et al. FGF23 decreases renal NaPi-2a and NaPi-2c expression and induces hypophosphatemia in vivo predominantly via FGF receptor 1. Am. J. Physiol. Ren. Physiol.297, F282–F291 (2009).
Saleh, M. et al. Abstract CT111: preliminary results from a phase 1/2 study of INCB054828, a highly selective fibroblast growth factor receptor (FGFR) inhibitor, in patients with advanced malignancies. Cancer Res.77, CT111–CT111 (2017).
Papadopoulos, K. P. et al. A Phase 1 study of ARQ 087, an oral pan-FGFR inhibitor in patients with advanced solid tumours. Br. J. Cancer117, 1592–1599 (2017).
Mazzaferro, V. et al. ARQ 087, an oral pan-fibroblast growth factor receptor (FGFR) inhibitor, in patients (pts) with advanced intrahepatic cholangiocarcinoma (iCCA) with FGFR2 genetic aberrations. J. Clin. Oncol.35, 4017–4017 (2017).
Goyal, L. et al. Polyclonal secondary FGFR2 mutations drive acquired resistance to FGFR inhibition in patients with FGFR2 fusion-positive cholangiocarcinoma. Cancer Discov.7, 252–263 (2017).
Kim, S. T. et al. Prospective blinded study of somatic mutation detection in cell-free DNA utilizing a targeted 54-gene next generation sequencing panel in metastatic solid tumor patients. Oncotarget6, 40360–40369 (2015).
Song, K. H., Li, T., Owsley, E., Strom, S. & Chiang, J. Y. Bile acids activate fibroblast growth factor 19 signaling in human hepatocytes to inhibit cholesterol 7alpha-hydroxylase gene expression. Hepatology49, 297–305 (2009).
Holt, J. A. et al. Definition of a novel growth factor-dependent signal cascade for the suppression of bile acid biosynthesis. Genes Dev.17, 1581–1591 (2003).
Arnold, A. et al. Genome wide DNA copy number analysis in cholangiocarcinoma using high resolution molecular inversion probe single nucleotide polymorphism assay. Exp. Mol. Pathol.99, 344–353 (2015).
Kaibori, M. et al. Increased FGF19 copy number is frequently detected in hepatocellular carcinoma with a complete response after sorafenib treatment. Oncotarget7, 49091–49098 (2016).
Luo, X. et al. Effectiveness and safety of sorafenib in the treatment of unresectable and advanced intrahepatic cholangiocarcinoma: a pilot study. Oncotarget8, 17246–17257 (2017).
Chakunta, H. R., Sunderkrishnan, R., Kaplan, M. A. & Mostofi, R. Cholangiocarcinoma: treatment with sorafenib extended life expectancy to greater than four years. J. Gastrointest. Oncol.4, E30–E32 (2013).
Borger, D. R. et al. Frequent mutation of isocitrate dehydrogenase (IDH)1 and IDH2 in cholangiocarcinoma identified through broad-based tumor genotyping. Oncologist17, 72–79 (2012).
Jiao, Y. et al. Exome sequencing identifies frequent inactivating mutations in BAP1, ARID1A and PBRM1 in intrahepatic cholangiocarcinomas. Nat. Genet.45, 1470–1473 (2013).
Wang, P. et al. Mutations in isocitrate dehydrogenase 1 and 2 occur frequently in intrahepatic cholangiocarcinomas and share hypermethylation targets with glioblastomas. Oncogene32, 3091–3100 (2013).
Zhu, A. X. et al. Genomic profiling of intrahepatic cholangiocarcinoma: refining prognosis and identifying therapeutic targets. Ann. Surg. Oncol.21, 3827–3834 (2014).
Yoshikawa, D. et al. Clinicopathological and prognostic significance of EGFR, VEGF, and HER2 expression in cholangiocarcinoma. Br. J. Cancer98, 418–425 (2008).
Lee, J. et al. Gemcitabine and oxaliplatin with or without erlotinib in advanced biliary-tract cancer: a multicentre, open-label, randomised, phase 3 study. Lancet Oncol.13, 181–188 (2012).
Borad, M. J. et al. Integrated genomic characterization reveals novel, therapeutically relevant drug targets in FGFR and EGFR pathways in sporadic intrahepatic cholangiocarcinoma. PLoS Genet.10, e1004135 (2014).
Li, M. et al. Whole-exome and targeted gene sequencing of gallbladder carcinoma identifies recurrent mutations in the ErbB pathway. Nat. Genet.46, 872–876 (2014).
Bekaii-Saab, T. et al. Multi-institutional phase II study of selumetinib in patients with metastatic biliary cancers. J. Clin. Oncol.29, 2357–2363 (2011).
Sullivan, R. J. et al. Atezolizumab (A) + cobimetinib (C) + vemurafenib (V) in BRAFV600-mutant metastatic melanoma (mel): updated safety and clinical activity. J. Clin. Oncol.35, 3063–3063 (2017).
Ewald, F. et al. Dual Inhibition of PI3K-AKT-mTOR- and RAF-MEK-ERK-signaling is synergistic in cholangiocarcinoma and reverses acquired resistance to MEK-inhibitors. Invest. New Drugs32, 1144–1154 (2014).
Yakes, F. M. et al. Cabozantinib (XL184), a novel MET and VEGFR2 inhibitor, simultaneously suppresses metastasis, angiogenesis, and tumor growth. Mol. Cancer Ther.10, 2298–2308 (2011).
Riener, M. O., Bawohl, M., Clavien, P. A. & Jochum, W. Rare PIK3CA hotspot mutations in carcinomas of the biliary tract. Genes Chromosomes Cancer47, 363–367 (2008).
Yeung, Y. et al. K-Ras mutation and amplification status is predictive of resistance and high basal pAKT is predictive of sensitivity to everolimus in biliary tract cancer cell lines. Mol. Oncol.11, 1130–1142 (2017).
Ahn, D. H. et al. Results of an abbreviated phase-II study with the Akt inhibitor MK-2206 in patients with advanced biliary cancer. Sci. Rep.5, 12122 (2015).
Zhang, Y. et al. A novel PI3K/AKT signaling axis mediates Nectin-4-induced gallbladder cancer cell proliferation, metastasis and tumor growth. Cancer Lett.375, 179–189 (2016).
Challita-Eid, P. M. et al. Enfortumab vedotin antibody-drug conjugate targeting nectin-4 is a highly potent therapeutic agent in multiple preclinical cancer models. Cancer Res.76, 3003–3013 (2016).
Ross, J. S. et al. New routes to targeted therapy of intrahepatic cholangiocarcinomas revealed by next-generation sequencing. Oncologist19, 235–242 (2014).
Tadokoro, H., Shigihara, T., Ikeda, T., Takase, M. & Suyama, M. Two distinct pathways of p16 gene inactivation in gallbladder cancer. World J. Gastroenterol.13, 6396–6403 (2007).
Kagohara, L. T. et al. Global and gene-specific DNA methylation pattern discriminates cholecystitis from gallbladder cancer patients in Chile. Future Oncol.11, 233–249 (2015).
Ahn, D. H. et al. Next-generation sequencing survey of biliary tract cancer reveals the association between tumor somatic variants and chemotherapy resistance. Cancer122, 3657–3666 (2016).
Golan, T. et al. Overall survival and clinical characteristics of BRCA-associated cholangiocarcinoma: A Multicenter Retrospective Study. Oncologist22, 804–810 (2017).
Yang, B., House, M. G., Guo, M., Herman, J. G. & Clark, D. P. Promoter methylation profiles of tumor suppressor genes in intrahepatic and extrahepatic cholangiocarcinoma. Mod. Pathol.18, 412 (2004).
Okaro, A. C., Deery, A. R., Hutchins, R. R. & Davidson, B. R. The expression of antiapoptotic proteins Bcl-2, Bcl-X(L), and Mcl-1 in benign, dysplastic, and malignant biliary epithelium. J. Clin. Pathol.54, 927–932 (2001).
Isomoto, H. et al. Sustained IL-6/STAT-3 signaling in cholangiocarcinoma cells due to SOCS-3 epigenetic silencing. Gastroenterology132, 384–396 (2007).
Yoon, J. H. et al. Bile acids inhibit Mcl-1 protein turnover via an epidermal growth factor receptor/Raf-1-dependent mechanism. Cancer Res.62, 6500–6505 (2002).
Wang, W. et al. FXR agonists enhance the sensitivity of biliary tract cancer cells to cisplatin via SHP dependent inhibition of Bcl-xL expression. Oncotarget7, 34617–34629 (2016).
Imamura, F. et al. Monitoring of treatment responses and clonal evolution of tumor cells by circulating tumor DNA of heterogeneous mutant EGFR genes in lung cancer. Lung Cancer94, 68–73 (2016).
Sato, T. et al. Long-term expansion of epithelial organoids from human colon, adenoma, adenocarcinoma, and Barrett’s epithelium. Gastroenterology141, 1762–1772 (2011).
Hyman, D. M. et al. The efficacy of larotrectinib (LOXO-101), a selective tropomyosin receptor kinase (TRK) inhibitor, in adult and pediatric TRK fusion cancers. J. Clin. Oncol.35, LBA2501–LBA2501 (2017).
Drilon, A. et al. Safety and antitumor activity of the multitargeted Pan-TRK, ROS1, and ALK inhibitor entrectinib: combined results from two phase ITrials (ALKA-372-001 and STARTRK-1). Cancer Discov.7, 400–409 (2017).
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
Reageer op "Personalised medicine op basis van DNA en RNA mutaties voor bv. immuuntherapie met anti-PD en gerichte behandelingen lijkt voor galwegenkanker zeker zinvol aldus overzichtsstudie"



Plaats een reactie ...
Reageer op "Personalised medicine op basis van DNA en RNA mutaties voor bv. immuuntherapie met anti-PD en gerichte behandelingen lijkt voor galwegenkanker zeker zinvol aldus overzichtsstudie"